Downloaded 15 times



![AMA Letter to CMMS and ONC
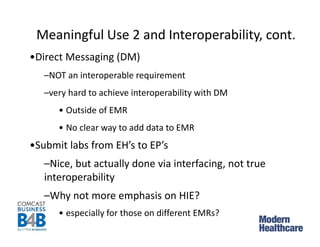
“JASON2 report funded by the Agency for Healthcare Research
and Quality concisely described the current state of
interoperability, finding “[a]t present, large-scale interoperability
amounts to little more than replacing fax machines with the
electronic delivery of page-formatted medical records.”3 If we
are to move away from this approach, the certification process
must be keenly focused on achieving true interoperability that is
deployed in a fashion that requires minimal user intervention.
We believe ONC should focus less on what specific data points
are exchanged, and more on identifying and coordinating the
standards needed to exchange information.”
• Lack of interoperability standards still impedes progress
1http://www.ihealthbeat.org/~/media/Files/2014/PDFs/CMS%20ONC%20Letter%20Stage%203.
ashx
2named for the Greek hero
3JASON, A Robust Health Data Infrastructure, November 2013
http://www.healthit.gov/sites/default/files/ptp13-700hhs_white.pdf](https://image.slidesharecdn.com/may21final-140520201428-phpapp01/85/Webinar-Information-Technology-How-to-achieve-interoperability-across-the-continuum-of-care-13-320.jpg)


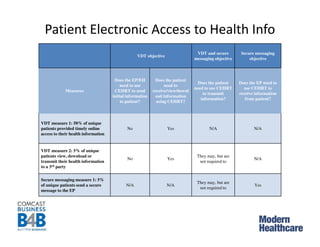
The document discusses health IT and achieving interoperability in care transitions, emphasizing the importance of electronic health record compliance and patient access to health information. It highlights various measures under meaningful use certifications and challenges such as the lack of interoperability standards and the complexity of current health information exchanges. The discussion also addresses recommendations for improved software architecture and the roles of participating health organizations.



































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)



