Download to read offline


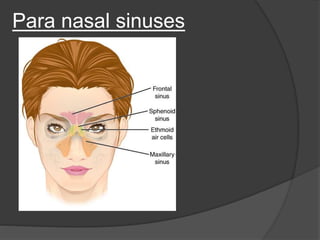
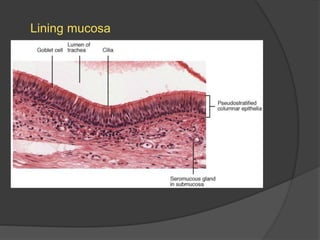
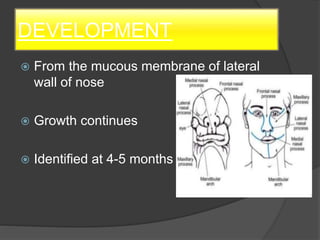
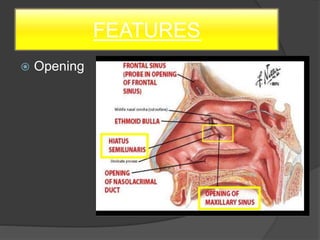
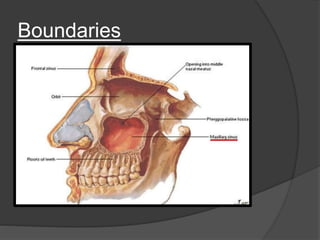
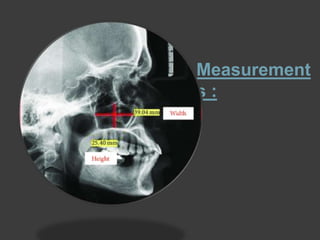
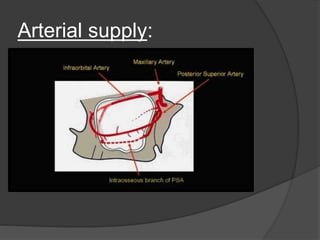
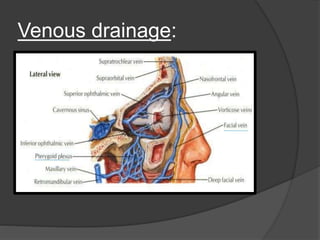
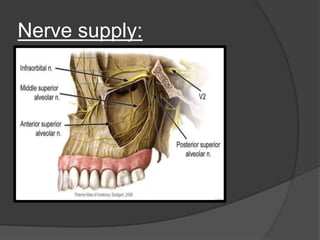
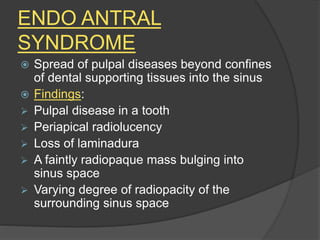

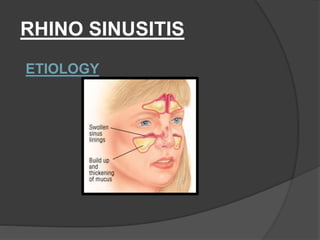
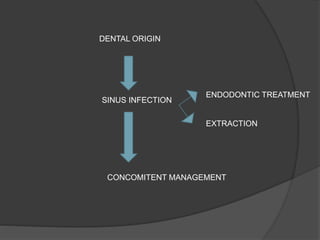
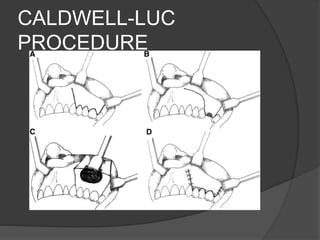


The document discusses the anatomy and development of the maxillary sinus, along with its applied aspects, including endodontic treatments and their complications. It highlights the relationship between maxillary sinus issues and dental conditions, emphasizing the importance of accurate diagnosis to differentiate between sinus pain and odontalgia. The conclusion stresses that conventional endodontic treatment is usually the best option for dental origin sinusitis, while surgical intervention may be needed for refractory cases.





























![final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/finalautosaved-221213152722-dbd9357e-thumbnail.jpg?width=640&height=640&fit=bounds)



















































