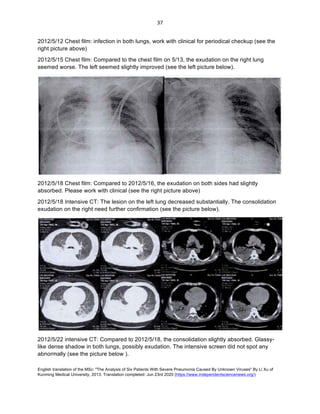
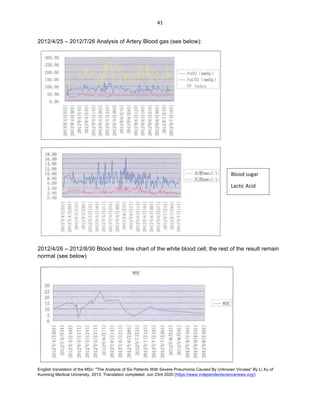
The document summarizes a case study of patient Zhou, a 63-year-old male mine worker admitted to the hospital with severe pneumonia of unknown cause. He had been exposed to bats and bat droppings in the mine where he worked. Over the course of his illness and treatment in the hospital, imaging showed worsening lung involvement and fluid buildup. Blood tests detected elevated inflammatory markers and abnormal liver and kidney function. Despite treatment, his condition deteriorated and he ultimately succumbed to the unknown illness.