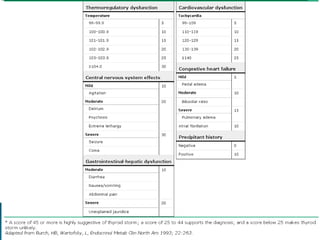
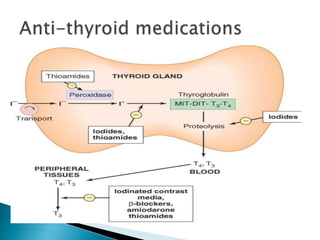
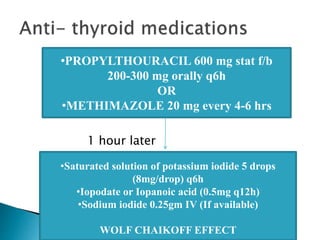
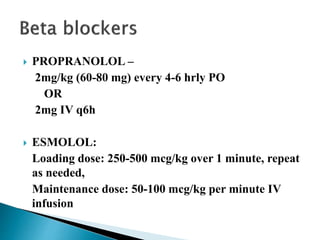
This document discusses thyroid storm, which is a life-threatening exacerbation of hyperthyroidism. It can have a mortality rate of 20-30%. Causes include infections, discontinuing thyroid medications, and other systemic stresses. Patients experience high metabolism, tachycardia, hypertension, and other symptoms. Treatment involves medications to stop thyroid hormone synthesis and block peripheral effects, supportive care, treating any precipitating causes, and monitoring for complications. Early diagnosis and aggressive treatment are needed to reduce mortality from this medical emergency.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










