Heart Failure inDiabetes: The
Role of SGLT2I
Dr. P. Suresh Kumar MD DM
Assistant professor of cardiology
Chengalpattu medical college
2.
Learning Objectives
• Understanddefinitions and epidemiology of HF in diabetes
• Review HF types & pathophysiology
• Examine mechanisms linking diabetes to HF
• Review evidence for SGLT2 inhibitors and CV outcomes
• Summarize major trials and clinical implications
3.
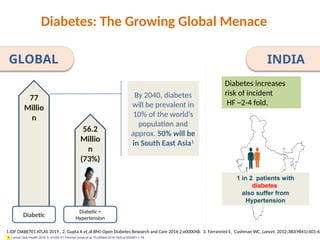
By 2040, diabetes
willbe prevalent in
10% of the world’s
population and
approx. 50% will be
in South East Asia1
Diabetes: The Growing Global Menace
1.IDF DIABETES ATLAS 2019 , 2. Gupta A et.al BMJ Open Diabetes Research and Care 2014;2:e000048. 3. Ferrannini E, Cushman WC. Lancet. 2012;380(9841):601-61
Diabetic
77
Millio
n
56.2
Millio
n
(73%)
Diabetic +
Hypertension
1 in 2 patients with
diabetes
also suffer from
Hypertension
INDIA
4. Lancet Glob Health 2018; 6: e1339–51 Prenissl Jonas et al. PLoSMed 2019;16(5):e1002801:1-18
GLOBAL
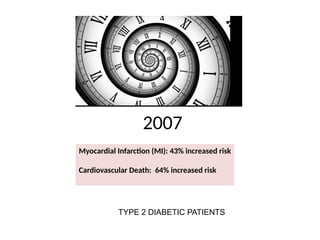
Diabetes increases
risk of incident
HF ~2-4 fold.
4.
Heart Failure andMortality
1/3 will die within 6 months of
hospitalisation for heart failure
Thereafter 5-10% die every year
5.
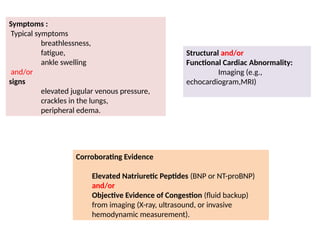
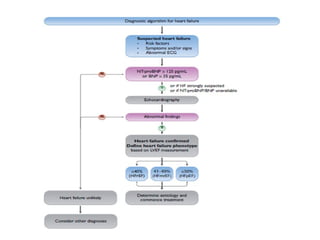
Definition of HeartFailure
Clinical syndrome with symptoms and/or signs
caused by a structural and/or functional cardiac
abnormality and corroborated by elevated natriuretic
peptide levels and/or objective evidence of pulmonary
or systemic congestion..
6.
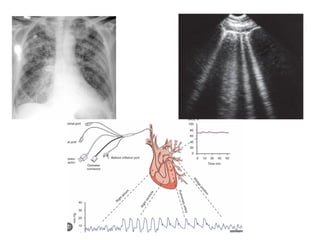
Symptoms :
Typical symptoms
breathlessness,
fatigue,
ankleswelling
and/or
signs
elevated jugular venous pressure,
crackles in the lungs,
peripheral edema.
Structural and/or
Functional Cardiac Abnormality:
Imaging (e.g.,
echocardiogram,MRI)
Corroborating Evidence
Elevated Natriuretic Peptides (BNP or NT-proBNP)
and/or
Objective Evidence of Congestion (fluid backup)
from imaging (X-ray, ultrasound, or invasive
hemodynamic measurement).
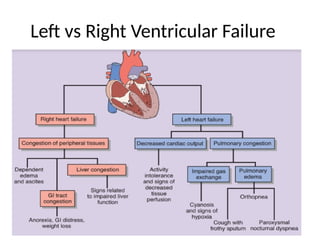
Left vs RightVentricular Failure
• Left ventricular failure: pulmonary congestion, dyspnea.
• Right ventricular failure: systemic venous congestion,
peripheral edema.
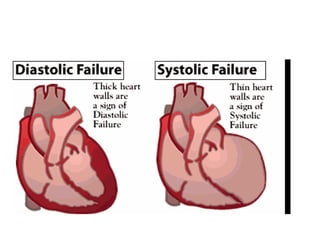
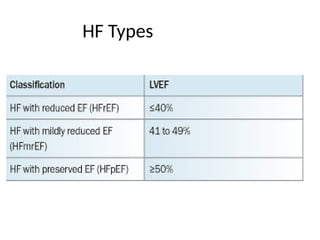
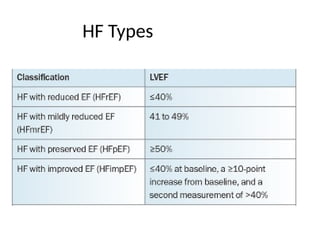
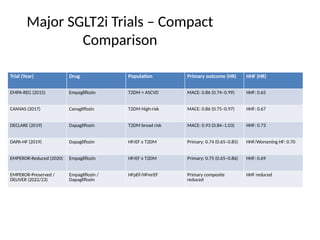
Heart Failure withReduced Ejection Fraction
(HFrEF), with or without Diabetes
2019
26% reduction
primary composite endpoint
(CV Death or Worsening HF Event).
DAPA-HF
Dapagliflozin
42.
Heart Failure withReduced Ejection
Fraction (HFrEF), with or without T2DM.
2020
EMPEROR-Reduced
Empagliflozin
25% reduction in the composite
endpoint (CV Death or HHF)
43.
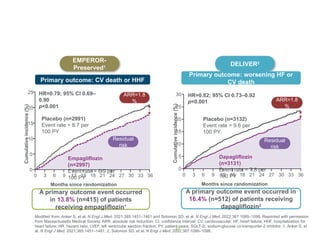
Heart Failure withPreserved Ejection
Fraction (HFpEF), with or without T2DM
First trial to successfully meet its primary
endpoint in HFpEF
2021
EMPEROR-Preserved
Empagliflozin
44.
Heart Failure withPreserved/Mildly Reduced
Ejection Fraction (HFpEF/HFmrEF), with or
without T2DM
2022
DELIVER
Dapagliflozin
Confirmed the benefit of SGLT2i in
HFpEF/HFmrEF,
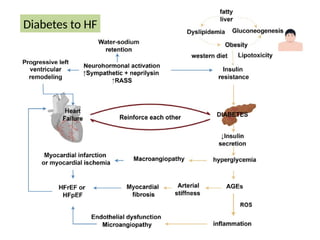
#25 Mechanism of Heart Failure Due to Diabetes Mellitus
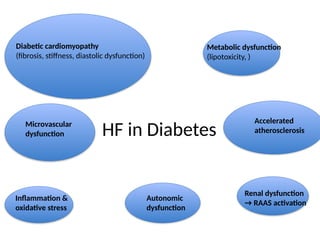
The pathophysiological mechanisms between DM and HF are complex and multifactorial.
Hyperglycemia, insulin resistance and hyperinsulinemia all seem to provoke and
perpetuate the progression of HF, though the exact mechanisms are unclear [28]. Excessive
production and accumulation of AGEs in plasma and vascular tissues lead to arterial stiffness
and reduced elasticity [29]. Meanwhile, AGE accumulation triggers the production of
reactive oxygen species (ROS), leading to myocardial and microcirculatory inflammation,
mitochondrial dysfunction and myocardial apoptosis. Additionally, chronic hyperglycemia
and insulin resistance may cause direct damage to the myocardium, along with the associated
metabolic abnormalities, promoting the development of atherosclerosis and vascular
damage. Hyperglycemia contributes to disturbed energy metabolism, inappropriate lipid
deposition in extra-adipose tissues (including epicardium) [30] and lipotoxicity, provoking
cardiomyocyte damage and triggering myocardial stiffness and ischemia [31]. Eventually,
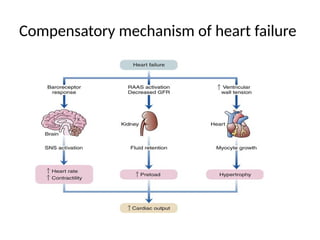
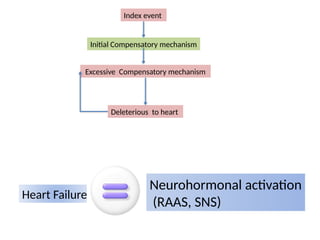
HF leads to renin–angiotensin–aldosterone system (RAAS) and sympathetic nervous system
activation. When coupled with the typical Western diet, obesity and fatty liver, HF
aggravates insulin resistance, and thus begins a vicious cycle [32] (Figure 2).
Biomedicines 2024, 12, 1572 4 of 20
studies directly compare the prevalence and incidence of DM in HFrEF and HFpEF patients,
in a study of inpatients with HF, the prevalence of DM was approximately 40% in
both HFrEF and HFpEF patients [27].
4.1. Mechanism of Heart Failure Due to Diabetes Mellitus
The pathophysiological mechanisms between DM and HF are complex and multifactorial.
Hyperglycemia, insulin resistance and hyperinsulinemia all seem to provoke and
perpetuate the progression of HF, though the exact mechanisms are unclear [28]. Excessive
production and accumulation of AGEs in plasma and vascular tissues lead to arterial
stiffness and reduced elasticity [29]. Meanwhile, AGE accumulation triggers the production
of reactive oxygen species (ROS), leading to myocardial and microcirculatory inflammation,
mitochondrial dysfunction and myocardial apoptosis. Additionally, chronic hyperglycemia
and insulin resistance
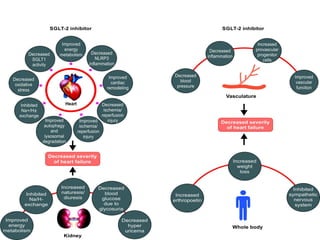
#40 Empagliflozin Suppression of the mTORC Pathway – enhanced oxidative phosphorylation- reduced hypertrophy and cardiac stiffness
Empagliflozin Regulation of Calcium Within Myocytes- inhibition of CaMK II – slows loss of Ca from SR
Empagliflozin Natriuretic and Diuretic Effects
Reduces interstitial fluid by 5.2% - hemoconc – increased O2 supply to myocardium
the cardiac benefits of
empagliflozin are due to improvement in myocardial
energetics via switching myocardial fuel metabolism
away from glucose to ketone bodies, which ameliorates
adverse LV remodeling.
Myocardial metabolic remodeling is integral
to HF development , with a shift from
free fatty acids (FFA) utilization toward glucose consumption
in failing hearts.
Protects endothelial glycocalx – reduces atherosclerosis