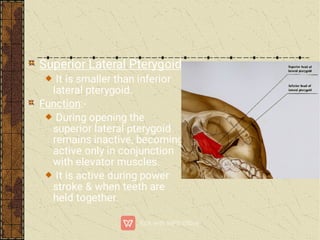
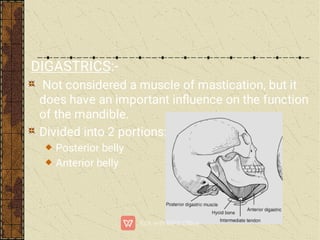
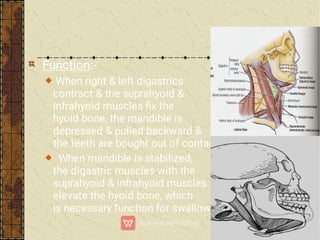
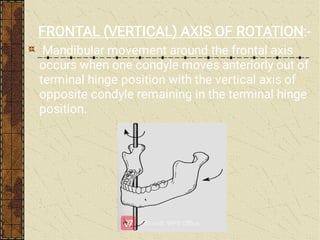
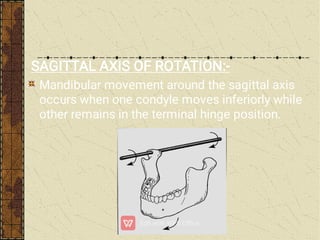
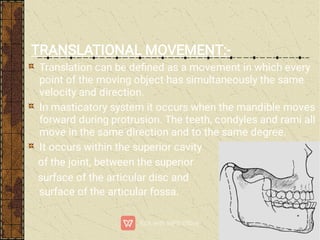
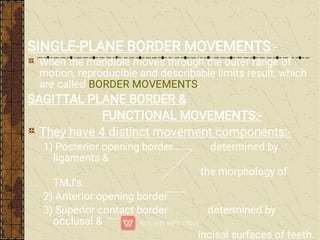
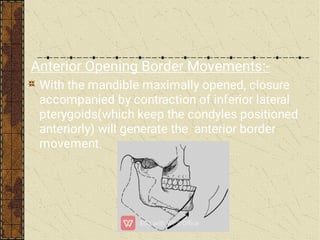
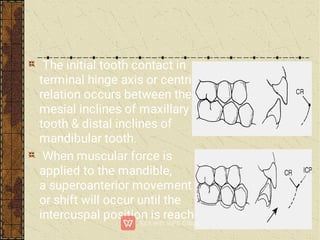
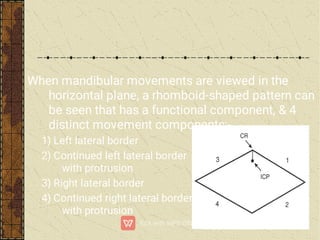
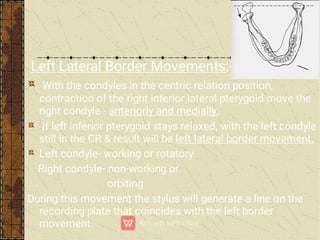
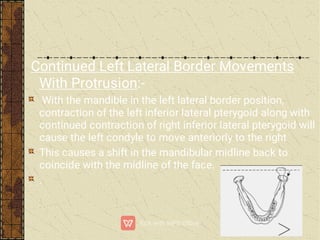
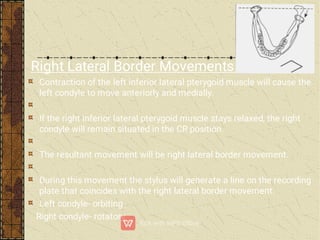
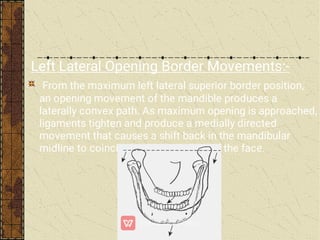
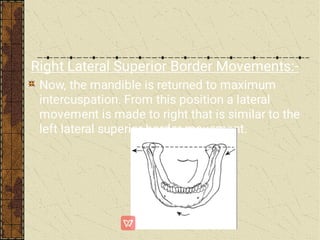
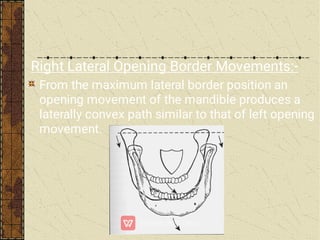
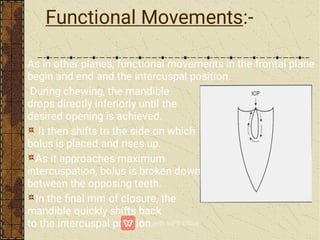
The document provides an extensive overview of mandibular movements, emphasizing the complexity of the masticatory system, which includes the maxilla, mandible, the temporomandibular joint (TMJ), and associated muscles. It discusses studies on the functionality of various muscles during jaw movements, the anatomy of the TMJ, and the roles of different ligaments and neurologic structures in controlling these movements. Additionally, it outlines methods for recording these movements and the significance of understanding them for dental practice and prosthesis design.