
Recommended
More Related Content
What's hot
What's hot (20)
Similar to management of endometrial_hyperplasia 2016_ small one water mark.pdf
Similar to management of endometrial_hyperplasia 2016_ small one water mark.pdf (20)
Recently uploaded
Recently uploaded (20)
management of endometrial_hyperplasia 2016_ small one water mark.pdf
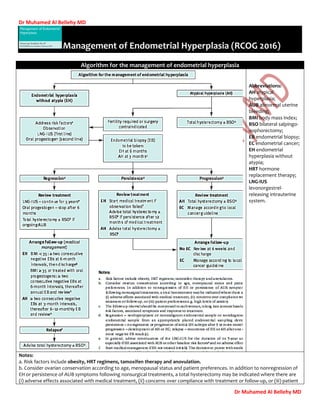
- 1. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD Management of Endometrial Hyperplasia (RCOG 2016) Algorithm for the management of endometrial hyperplasia Abbreviations: AH atypical hyperplasia; AUB abnormal uterine bleeding; BMI body mass index; BSO bilateral salpingo- oophorectomy; EB endometrial biopsy; EC endometrial cancer; EH endometrial hyperplasia without atypia; HRT hormone replacement therapy; LNG-IUS levonorgestrel- releasing intrauterine system. Notes: a. Risk factors include obesity, HRT regimens, tamoxifen therapy and anovulation. b. Consider ovarian conservation according to age, menopausal status and patient preferences. In addition to nonregression of EH or persistence of AUB symptoms following nonsurgical treatments, a total hysterectomy may be indicated where there are (i) adverse effects associated with medical treatment, (ii) concerns over compliance with treatment or follow-up, or (iii) patient
- 2. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD preferences e.g. high levels of anxiety. c. The follow-up interval should be customised to each woman, taking into account baseline risk factors, associated symptoms and response to treatment. d. Regression – nonhyperplastic or nonmalignant endometrial sample or nondiagnostic endometrial sample from an appropriately placed endometrial sampling device; persistence – no regression or progression of initial EH subtype after 3 or more months; progression – development of AH or EC; relapse – recurrence of EH or AH after one or more negative EB result(s). e. In general, advise continuation of LNG-IUS for duration of its 5-year use, especially if EH associated with AUB or other baseline risk factorsa and no adverse effects. f. Start medical management if EH not treated initially. The decision to persist with medical management should be taken after careful consideration and thorough discussion with the woman regarding the risks and benefits of prolonged medical treatment compared with total hysterectomy ± BSO. Persistence beyond 12 months is associated with a significant risk of underlying malignancy and a high risk of failure to regress such that a total hysterectomy ± BSO should be recommended. g. At discharge, inform the woman of her estimated individual risk of recurrence, of the need to continue any risk-reducing strategies and to present for an urgent review if any further episodes of AUB. h. Review the appropriateness of ongoing endometrial surveillance, continuation of medical management or total hysterectomy ± BSO based on factors such as baseline risk factors including BMI, AUB symptoms, fertility requirements, compliance with treatment and follow-up, medical comorbidities and risk–benefit ratio for total hysterectomy ± BSO. Endometrial hyperplasia (EH) is defined o as irregular proliferation of the endometrial glands with an increase in the gland to stroma ratio when compared with proliferative endometrium. Endometrial cancer is the most common gynaecological malignancy in the Western world and endometrial hyperplasia is its precursor. The most common presentation of endometrial hyperplasia is abnormal uterine bleeding (AUB). This includes o heavy menstrual bleeding (HMB), o intermenstrual bleeding, o irregular bleeding, o unscheduled bleeding on hormone replacement therapy (HRT) o postmenopausal bleeding (PMB). risk factors for endometrial hyperplasia? the main risk factor unopposed estrogen Known risk factors that reflect this aetiology: o increased BMI excessive peripheral conversion of androgens in adipose tissue to estrogen Obesity (a major risk factor) advise women to lose weight_ bariatric surgery may reduce this risk. severely obese women up to 10% asymptomatic EH o anovulation: associated with the perimenopause or PCOS likely to regress to normal once women with PCOS resume ovulation or perimenopausal women reach the menopause; o estrogen-secreting ovarian tumours e.g. granulosa cell tumours (40% prevalence of EH) o Drug-induced endometrial stimulation: unopposed systemic estrogen HRT in women with a uterus combined HRT regimen alone is often sufficient in inducing regression of EH without atypia. over-the-counter preparations that may contain high potency estrogens. long-term tamoxifen other factors immunosuppression and infection.
- 3. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD o As renal graft recipients renal graft recipients + AUB a 2-fold increased incidence of eh compared with nontransplanted controls How should endometrial hyperplasia be classified 1994 WHO classification o based upon complexity of the glandular architecture and presence of nuclear atypia. o It comprised 4 categories: (i) simple hyperplasia, (ii) complex hyperplasia, (iii) simple hyperplasia with atypia (iv) complex hyperplasia with atypia. The endometrial intraepithelial neoplasia (EIN) classification 2003 o The EIN diagnostic schema comprises 3 categories – benign (endometrial hyperplasia), premalignant (a diagnosis of EIN based upon 5 subjective histological criteria) malignant (endometrial cancer) – o this classification is not extensively used in the UK. The revised 2014 World Health Organization (WHO) classification is recommended. o based upon the presence of cytological atypia hyperplasia without atypia atypical hyperplasia. o the complexity of architecture is no longer part of the classification. o Dx of EIN aka atypical hyperplasia. workup (Endometrial tissue specimens/ Endometrial sampling) o DX requires histological examination of the endometrial tissue. o are obtained either by Outpatient endometrial biopsy: miniature outpatient suction devices that blindly abrade and/or aspirate endometrial tissue from the uterine cavity it is convenient _ high accuracy for diagnosing endometrial cancer. o The accuracy for hyperplasia is more modest negative result 2% have EH. inpatient endometrial sampling, such as D & C performed under general anaesthesia. Diagnostic hysteroscopy Direct visualization and biopsy to facilitate or obtain an endometrial sample, where outpatient sampling fails or is nondiagnostic For a polyp or other focal lesion A transvaginal ultrasound scan (TVS) o detects an irregularity of endometrial profile or an abnormal double layer endometrial thickness measurement perform an endometrial biopsy o in PMB
- 4. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD when the endometrial thickness is less than the cut-off 3 mm or 4 mm probability of cancer < 1% a larger cut-off value has been suggested for HRT or tamoxifen, whether presenting with AUB or asymptomatic. o in premenopausal women TVS is less sensitive to identifying EH or Ca for PCOS + absent withdrawal bleeds or AUB RCOG TVS endometrial thickness < 7 mm below this cut-off EH is unlikely. o TVS to exclude the possibility of granulosa cell tumour of the ovary. If an ovarian cyst ovarian tumour markers serum inhibin & estradiol if a granulosa cell tumour is suspected. Hysteroscopy o When Hysteroscopy allows additional endometrial assessment that may be necessary if abnormal bleeding persists or if intrauterine structural abnormalities such as polyps are suspected on TVS or endometrial biopsy where sampling is not possible or is nondiagnostic Directed biopsies o Advantages Hysteroscopy can detect focal lesions such as polyps that may be missed by blind sampling o outpatient sampling. o inpatient endometrial sampling up to 10% of endometrial pathology can be missed repeated curettage should be minimised to reduce incidence of Asherman’s syndrome. Diagnostic hysteroscopy can be conducted in the outpatient setting without the need for anaesthesia o The accuracy of hysteroscopy in diagnosing cancer and hyperplasia in women with AUB hysteroscopy is more accurate in detecting than excluding endometrial disease and has a higher accuracy for endometrial cancer than endometrial hyperplasia. CT, diffusion-weighted MRI or biomarkers insufficient evidence evaluating them as aids in the management of endometrial hyperplasia their use is not routinely recommended. CT or MRI o CT scan a preoperative CT scan for AH or grade 1 endometrial cancer could alter management in 4.3%. not be routinely recommended. o Diffusion-weighted MRI (need more evidence) for it may help in identifying women with invasive cancer future potential to DX endometrial hyperplasia & other endometrial lesions. biomarkers yet none of them predicts disease or prognosis accurately enough to be clinically useful.
- 5. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD o phosphatase and tensin homolog (PTEN), perhaps in combination with B-cell lymphoma 2 (BCL- 2) and BCL-2-like protein 4 (BAX),. the natural history of hyperplasia without atypia and its risk for progression to cancer. regression to normal endometrium persistent EH Progressed simple hyperplasia 74-81% 17- 18% 9% progressed to AH after 24 weeks of follow- up 1% progressed to endometrial cancer after 12 years complex hyperplasia 75-79% 21-25% 3% progressed to endometrial cancer RCOG observation alone majority will regress Progestogens vs observation alone higher disease regression cumulative long-term risk for progression to cancer is < 5% over 20 years For AH risk of endometrial cancer is > EH _ in 4 yrs 8%, 12.4% after 9 years and to 27.5% after 19 years. associated with a rate of concomitant carcinoma of up to 43% in women undergoing hysterectomy Management of endometrial hyperplasia Treatment o the first-line medical treatment Observation alone with follow-up endometrial biopsies to ensure disease regression, especially when identifiable risk factors can be reversed. Progestogen treatment is indicated in women who fail to regress following observation alone and in symptomatic women (AUB). Reversible risk factors should be identified and addressed. Observation alone is expected to fail where there is no identifiable reversible risk factor causing the endometrial hyperplasia, (limited evidence) o women with EH + AUB symptomatic treatment o surgical management for EH Hysterectomy observation only vs Progestogen treatment the first-line medical treatment progestogens (Effect of Progestogens modify the proliferative effects of estrogen on the endometrium) o continuous oral progestogens should be used for women who decline the LNG-IUS
- 6. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD Cyclical progestogens should not be used because they are less effective in inducing regression compared with continuous oral progestogens or LNG-IUS. Such as norethisterone (NET), MPA & megestrol acetate. significant adverse effects & norethisterone at a high dose has similar contraindications to COCs. disease regression rates were similar for all drugs. MPA (10–20 mg/day) & NET (10–15 mg/day). o local intrauterine [LNG-IUS] progestogens. the first-line medical treatment because compared with oral progestogens it has a higher disease regression rate less likely to need hysterectomy RCT LNG-IUS VS oral continuous medroxyprogesterone Regression rate After 3 months Regression rate After 6 months LNG-IUS 84% 100% oral MPA 50% 64% recommended as first-line treatment for HMB.--> a more favourable bleeding profile _ a higher concentration of levonorgestrel at the level of the endometrium provide effective contraception minimises systemic absorption of hormones adverse effects more compliance Duration of treatment & follow-up duration of treatment duration of treatment for oral progestogens For LNG-IUS 6 months up to 5 years Cessation after 3–6 months of therapy is commonly practiced, o may relate to fears over potential adverse effects from chronic administration of high-dose and compliance issues Endometrial surveillance By outpatient endometrial biopsy. o review schedules take into account presence of AUB Relapse higher risk of disease relapse, persistence or progression, BMI ≥ 35 or treated with oral progestogens relapse of complex EH following in 12.7% of treated with LNG-IUS vs 28.3% of treated with oral progestogens. over a median follow-up of 67 months for LNG-IUS o only 3% of women with a BMI < 35 relapsed during follow-up. o 33% of women with a BMI ≥ 35. surgical management for EH Hysterectomy Hysterectomy should not be considered as a first-line treatment o because progestogen therapy induces histological and symptomatic remission in the majority of women. Hysterectomy is indicated in women not wanting to preserve their fertility when (any of) o progression to AH occurs during follow-up, or o no histological regression of EH despite 12 months of treatment (then high cancer risk). small increase in overall regression rates of EH beyond 12 months of treatment
- 7. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD o relapse after completing progestogen treatment o persistence of bleeding symptoms, o woman declines to undergo endometrial surveillance or comply with medical treatment. Type ? o women with EH + Postmenopausal women total hysterectomy + BSO. For premenopausal women total hysterectomy ± BSO decision to remove ovaries should be individualised + consider bilateral salpingectomy (may reduce risk of a ovarian malignancy). approach A laparoscopic approach is preferable to an abdominal approach should be avoided o Supra cervical hysterectomy to ensure that all premalignant disease is eliminated. o Endometrial ablation is because complete & persistent endometrial destruction cannot be ensured_ and regeneration of ablated endometrial tissue may occur intrauterine adhesion formation may preclude endometrial histological surveillance. For AH Lymphadenectomy should not be routinely performed o because this would result in unnecessary surgical risk for the majority of women. When endometrial cancer found during hysterectomy was usually early stage with low risk of lymphovascular disease intraoperative frozen section of the endometrium no benefit_ not a reliable indicator of final pathology. What type of / method chosen for hysterectomy For women with AH o A laparoscopic approach is preferable to an abdominal approach as it is associated with a shorter hospital stay, less postoperative pain and quicker recovery. Due to the risks of disseminating malignancy, morcellation of the uterus should be avoided. allow staging _ some evidence o in all peri- and postmenopausal total hysterectomy + BSO. Due to the risk of underlying malignancy o For premenopausal total hysterectomy + individualized decision to remove ovaries + bilateral salpingectomy bilateral salpingectomy should be considered as this may risk of future ovarian malignancy. the risks of surgical menopause have to be balanced against the risk of underlying cancer and the need for further surgery to remove the ovaries. Premenopausal women who undergo total hysterectomy + BSO consider estrogen replacement, in absence of contraindications to its use, until the age of the natural menopause BSO is associated with increased mortality in women < 50 years who had hysterectomy for benign disease Fertility-sparing therapy in AH counselling o outcome for fertility one-quarter of women achieving a live birth o risks of underlying malignancy
- 8. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD progression to endometrial cancer. risk of relapse is uncertain pretreatment work-up o to rule out invasive endometrial cancer EB by hysteroscopy to minimise the chance of missing cancer or co-existing ovarian cancer. o MRI, CT, TVS and serum CA125 to rule out endometrial cancer or ovarian cancer. treatment o First-line treatment LNG-IUS o second-best alternative oral progestogens o Once fertility is no longer required hysterectomy should be offered (d2 high risk of disease relapse). Other hormonal therapies as a fertility-sparing treatment (The optimal treatment regimen is also ill-defined) o oral progestogens o LNG-IUS o aromatase inhibitors o gonadotrophin-releasing hormone agonists Followed up after fertility-sparing treatment (see investigations) + o TVS: 1. assessment of endometrial thickness unlikely to be useful in view of o the absence of validated reference ranges o the difficulty in obtaining accurate measurements with LNG-IUS in place. Outcome of fertility preservation o Failure to regress a worrying sign for underlying endometrial cancer. o relapse The risk of relapse is especially high in the first 2 years from diagnosis. If relapse occurs: hysterectomy should be strongly recommended o it is often associated with endometrial cancer at hysterectomy specimen. If this is not possible or declined further cycle of progestogen treatment. When to start fertility treatment? Disease regression (of AH or well-differentiated endometrial cancer) should on at least one endometrial sample before women attempt to conceive. initiate ART immediately following cessation of progestogen treatment o compared to natural conception as live birth rate is higher and it may prevent relapse Immediate ART avoids a prolonged interval of time without progestogen treatment o LBR_ 26.3% hyperplastic endometrium may predispose to infertility. A hysterectomy should be recommended to women with AH once fertility is no longer required because of the high relapse rate of disease and the potential for disease progression. HRT and endometrial hyperplasia Prevention
- 9. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD o All women taking HRT should be encouraged to report any unscheduled vaginal bleeding promptly. o Systemic estrogen-only HRT should not be used in women with a uterus. Women with endometrial hyperplasia + HRT _ who wish to continue HRT o For sequential HRT preparation offer change to continuous progestogen intake _ LNG-IUS or a continuous combined HRT prevalence of EH compared with sequential regimens (not statistically significant) Stopping sequential combined HRT may be sufficient to induce regression of endometrial hyperplasia o For continuous combined HRT Consider LNG-IUS as a source of progestogen replacement. Management of endometrial hyperplasia be managed in women on adjuvant treatment for breast cancer Risk of developing endometrial hyperplasia on adjuvant treatment for breast cancer Tamoxifen o a SERM that inhibits proliferation of breast cancer by competitive antagonism at E receptors. it has a partial agonist action on other tissues, including vagina and uterus may promote development fibroids, endometrial polyps & EH & risk of endometrial cancer Should women on tamoxifen be treated with prophylactic progestogen therapy Some evidence LNG-IUS prevents polyp formation & reduces incidence of EH Safety of LNG-IUS on breast cancer recurrence risk remains uncertain so its routine use cannot be recommended. risk increases with both dose and duration of treatment. Age varies between pre- and postmenopausal women. o risk of endometrial cancer was not statistically significant in women aged ≤ 49 years and a statistically significant in women aged ≥ 50 years Management of women who develop EH while on tamoxifen treatment need for tamoxifen should be reassessed management should be according to the histological classification aromatase inhibitors (such as anastrozole, exemestane and letrozole) Does not increase risk of EH and cancer or vaginal bleeding. have a similar regressing effect to tamoxifen explored as treatment for EH in small observational studies .Management of endometrial hyperplasia confined to an endometrial polyp Complete removal of the uterine polyp(s) +endometrial sample / biopsy + histological analysis from background endometrium_ even if the endometrium looks healthy on hysteroscopy o Concurrent endometrial hyperplasia in a polyp and the background endometrium 52%. slightly more likely for Women with AH in a polyp than those with hyperplasia without atypia Subsequent management should be according to the histological classification of endometrial hyperplasia. o atypia may be restricted to foci within the polyp + In absence of background EH.
- 10. Dr Muhamed Al Bellehy MD Dr Muhamed Al Bellehy MD removal of the polyp may be curative (very little evidence).