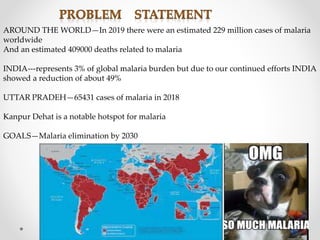
The document discusses malaria, detailing its epidemiological determinants, modes of transmission, and the impact of various Plasmodium species. It highlights India's status as representing 3% of the global malaria burden with a goal of malaria elimination by 2030, alongside important characteristics of susceptible populations and measurement indices for malaria control. Additionally, it outlines the stages of malaria infection and suggests various indices to monitor the disease's prevalence and control efforts.






































![Epidemiology of malaria [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/epidemiologyofmalariaautosaved-201006062122-thumbnail.jpg?width=640&height=640&fit=bounds)

































