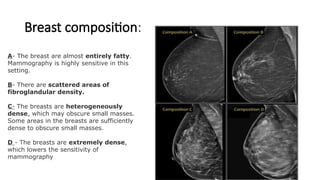
Breast composition:
A- Thebreast are almost entirely fatty.
Mammography is highly sensitive in this
setting.
B- There are scattered areas of
fibroglandular density.
C- The breasts are heterogeneously
dense, which may obscure small masses.
Some areas in the breasts are sufficiently
dense to obscure small masses.
D - The breasts are extremely dense,
which lowers the sensitivity of
mammography
3.
• Four mainlesions are visible mammographically:
1. Masses
2. Calcifications
3. Architectural distortion
4. Focal density
4.
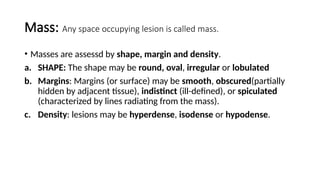
Mass: Any spaceoccupying lesion is called mass.
• Masses are assessd by shape, margin and density.
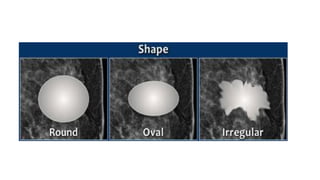
a. SHAPE: The shape may be round, oval, irregular or lobulated
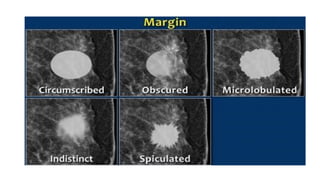
b. Margins: Margins (or surface) may be smooth, obscured(partially
hidden by adjacent tissue), indistinct (ill-defined), or spiculated
(characterized by lines radiating from the mass).
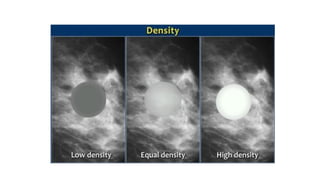
c. Density: lesions may be hyperdense, isodense or hypodense.
9.
Characteristics of benignand malignant
lesions:
• Benign lesions have following characteristics:
Shape: round or oval
margins: well-defined or smooth
density: hypodense
Malignant lesions may be:
Shape: irregular
margins: spiculated or irregular/indistinct
density: hyperdense
10.
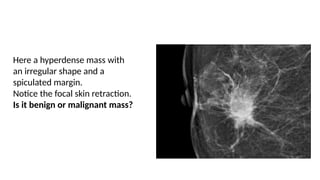
Here a hyperdensemass with
an irregular shape and a
spiculated margin.
Notice the focal skin retraction.
Is it benign or malignant mass?
11.
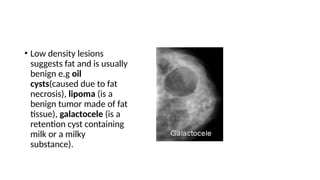
• Low densitylesions
suggests fat and is usually
benign e.g oil
cysts(caused due to fat
necrosis), lipoma (is a
benign tumor made of fat
tissue), galactocele (is a
retention cyst containing
milk or a milky
substance).
12.
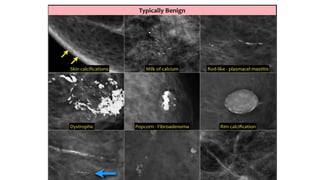
Calcifications:
• Calcifications varyin size, shape, number, grouping and orientation.
• Benign calcifications are:
dermal, vascular, popcorn, rod and ringlike calcifications
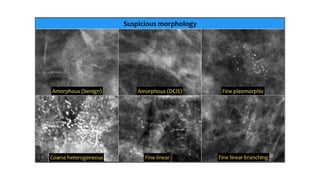
• Malignant calcification: grouped , liner or branching and irregular in
size, shape and separation.
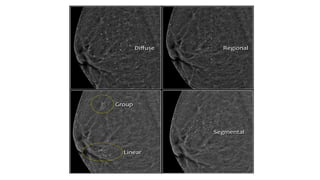
15.
Distribution of calcifications
Thearrangement of calcifications, the distribution, is at least as important as
morphology.
• These descriptors are arranged according to the risk of malignancy:
• Diffuse: distributed randomly throughout the breast.
• Regional: occupying a large portion of breast tissue > 2 cm greatest dimension
• Grouped (historically cluster): few calcifications occupying a small portion of breast tissue: lower
limit 5 calcifications within 1 cm and upper limit a larger number of calcifications within 2 cm.
• Linear: arranged in a line, which suggests deposits in a duct.
• Segmental: suggests deposits in a duct or ducts and their branches.
• The 2013 edition refines the upper limit in size for grouped distribution as 2 cm
(historically 1 cm) while retaining > 2 cm as the lower limit for regional distribution.
17.
Architectural distortion
• Theterm architectural distortion is used, when the normal architecture is distorted
with no definite mass visible.
• Architectural distortion may be associated with breast cancer because cancer
infiltration can disrupt parenchymal architecture before there is evidence of a mass.
• It may also be seen in areas of prior breast injury or surgery, which tend to improve
or remain unchanged over time.
• Therefore, comparison with previous mammographic findings (if available) is
essential.
• Another benign cause of architectural distortion is radial scar(a growth that looks like
a scar), which is a non-traumatic lesion.
• Unexplained architectural distortion warrants biopsy.
18.
Notice the distortionof the normal
breast architecture on oblique view
(yellow circle) and magnification
view.
A resection was performed and only
scar tissue was found in the
specimen.
19.
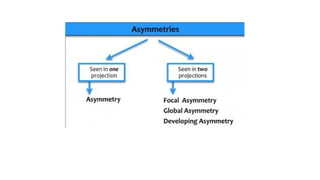
Asymmetries
• Findings thatrepresent unilateral deposits of fibro-glandulair tissue not
conforming to the definition of a mass are called asymmetries.
• Asymmetry as an area of fibroglandulair tissue visible on only one mammographic
projection, mostly caused by superimposition of normal breast tissue.
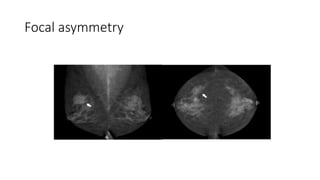
• Focal asymmetry visible on two projections, hence a real finding rather than
superposition.
• This has to be differentiated from a mass.
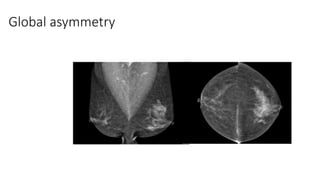
• Global asymmetry consisting of an asymmetry over at least one quarter of the
breast and is usually a normal variant.
• Developing asymmetry new, larger and more conspicuous than on a previous
examination.
Asymmetry versus Mass
•All types of asymmetry have different border contours than true
masses and also lack the conspicuity of masses.
• Asymmetries appear similar to other discrete areas of fibroglandulair
tissue except that they are unitaleral, with no mirror-image correlate in
the opposite breast.
• An asymmetry demonstrates concave outward borders and usually is
interspersed with fat, whereas a mass demonstrates convex outward
borders and appears denser in the center than at the periphery.
25.
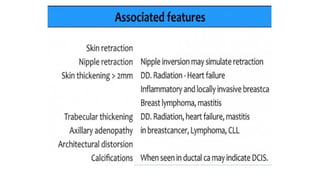
Other feautres:
• Associatedfeatures are things that are seen in association with
suspicious findings like masses, asymmetries and calcifications.
• Associated features such as skin thickening, skin retraction, nipple
retraction and trabecular thickening.
• These are assessed with the main features outlined above and in light
of clinical picture.
• Associated features play a role in the final assessment.