Downloaded 27 times










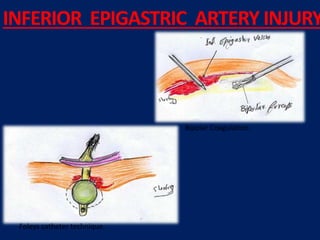




- Inserts a Foley catheter through the 5mm port - Inflates the balloon in the retroperitoneum - Compresses the bleeding vessel - Allows controlled deflation after haemostasis INFERIOR EPIGASTRIC ARTERY INJURY SECONDARY TROCAR INJURIES - Bowel injury - Vascular injury - Bladder injury - Ureteric injury Risk factors: - Poor technique - Adhesions - Obesity - Previous surgery Management: - Laparoscopic repair - Conversion to laparotomy SECONDARY TROCAR INJURIES HAND INSTRUMENT










































































