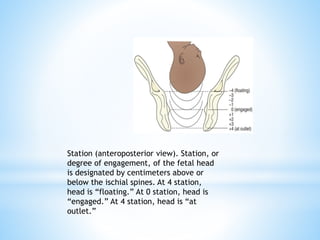
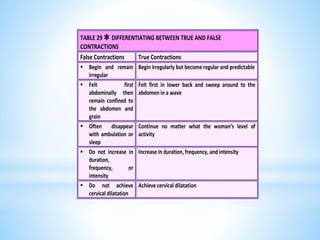
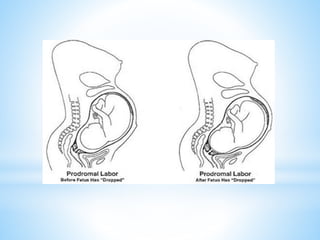
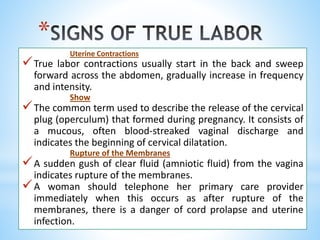
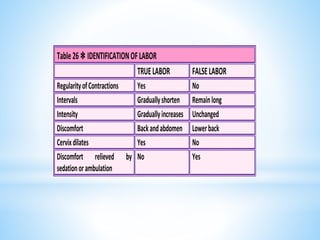
Labor normally begins when a fetus is sufficiently mature to survive outside the uterus, yet not too large to cause difficulties during birth. Contractions of the uterus and changes in the cervix prepare the body for delivery. Some signs that labor is imminent include lightening, increased energy, slight weight loss, backache, and Braxton Hicks contractions. True labor involves regular, intensifying uterine contractions and cervical changes like effacement and dilation that allow the baby to pass through the birth canal. Understanding the signs of true labor helps prevent premature birth and helps the woman recognize when labor begins.
![A.Fetal Position
the relationship of the fetal presenting part to a specific quadrant of the
woman’s pelvis.
For convenience, the maternal pelvis is divided into four quadrants
according to the mother’s right and left:
A. right anterior
B. left anterior
C. right posterior
D. left posterior.
Four parts of a fetus have been chosen as landmarks to describe the
relationship of the presenting part to one of the pelvic quadrants
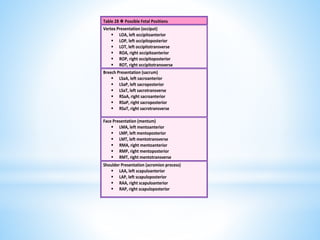
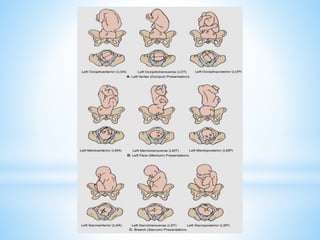
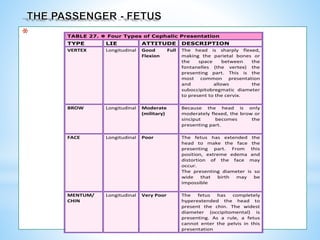
In a Vertex presentation, the occiput (O) is the chosen point
In a Face presentation, it is the chin (mentum [M])
In a Breech presentation it is the sacrum (Sa)
In a Shoulder presentation, it is the scapula or the acromion process. (A)
LETTERS ARE ABBREVIATED
The first letter denotes the mother’s right (R) or left (L)
The middle letter denotes fetal landmark
The last letter denotes the landmark points either anterior (A), posterior
(P) or transverse (T).
*](https://image.slidesharecdn.com/laboronsetoflabor-230118014953-92bd7a01/85/LABOR-ONSET-OF-LABOR-pptx-41-320.jpg)