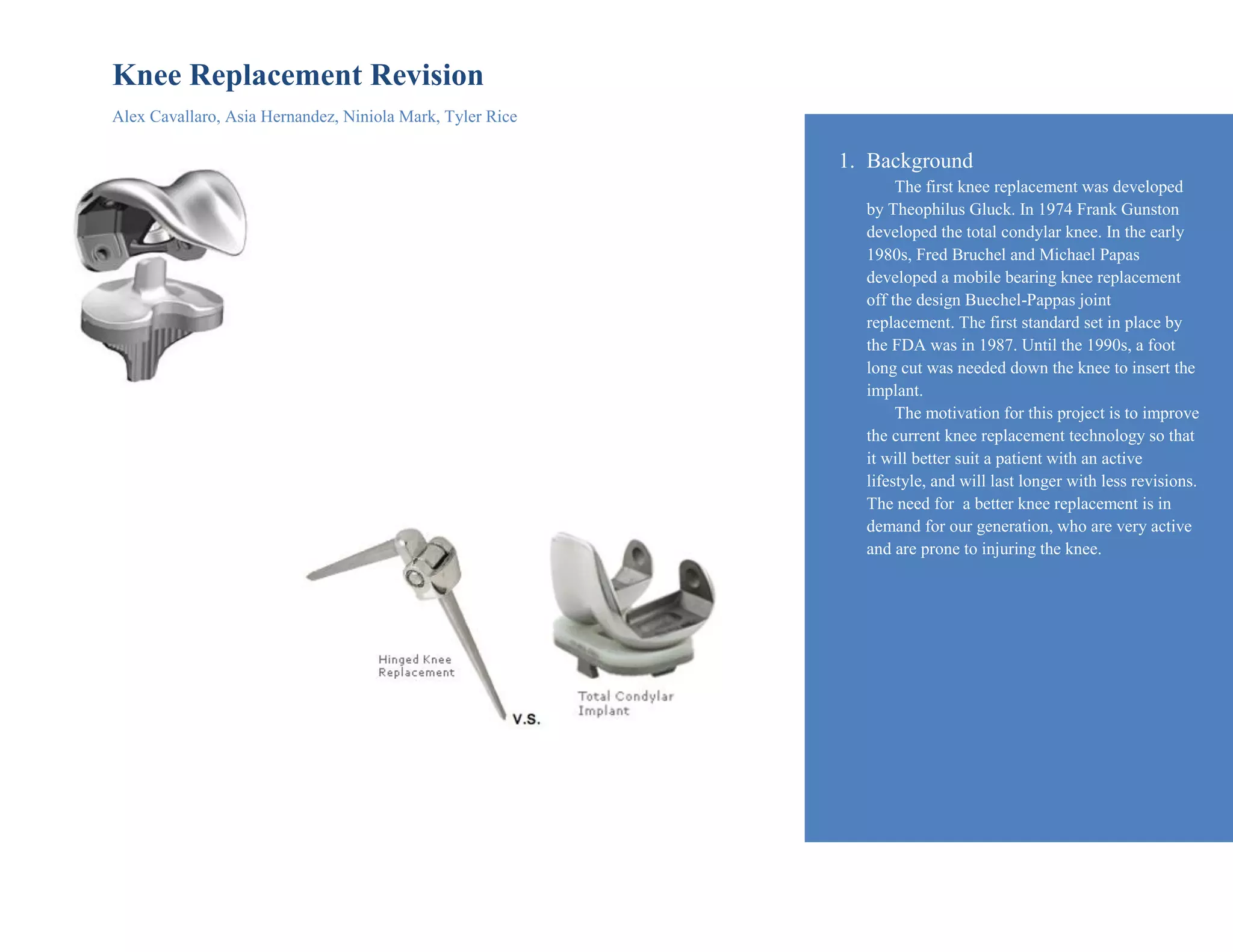
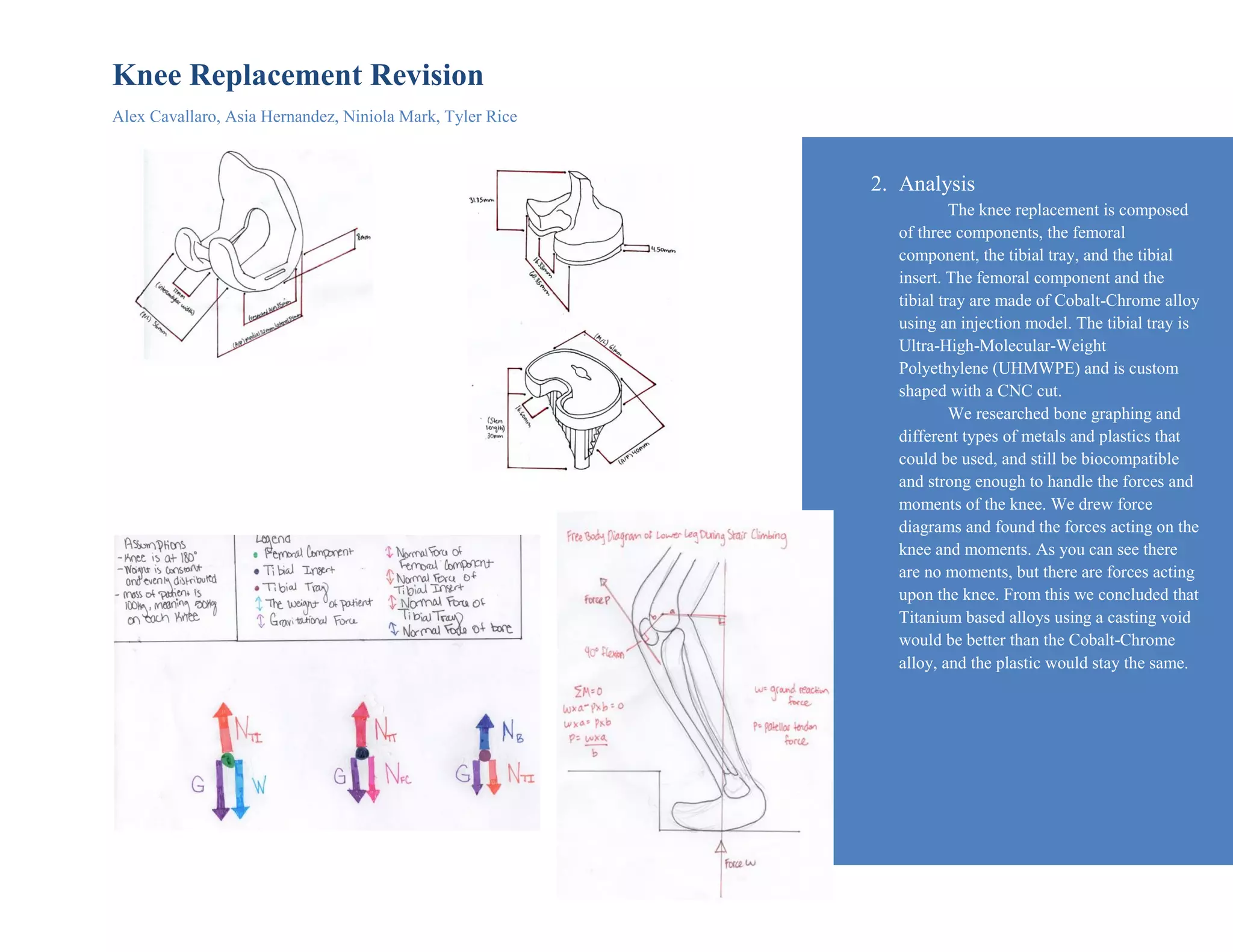
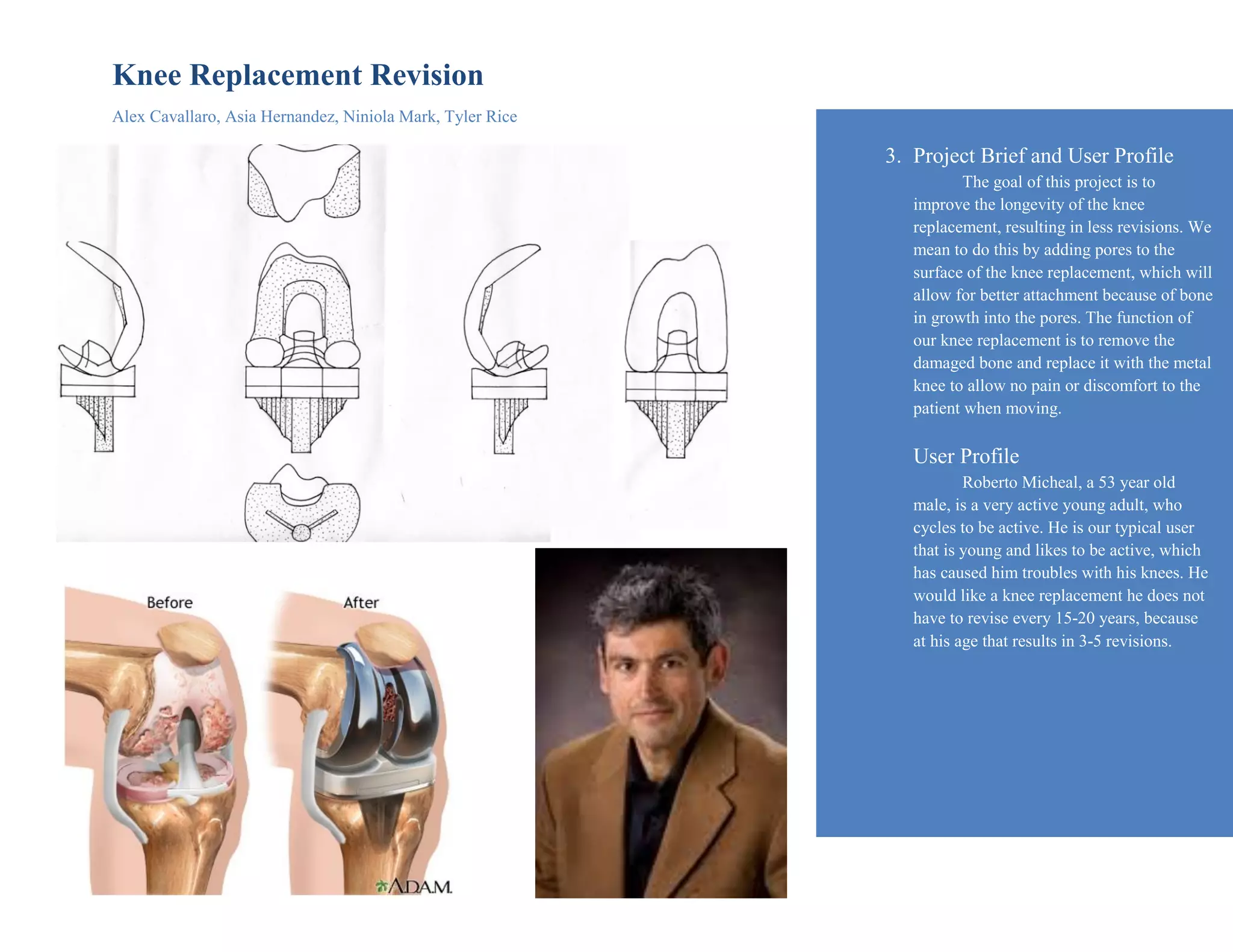
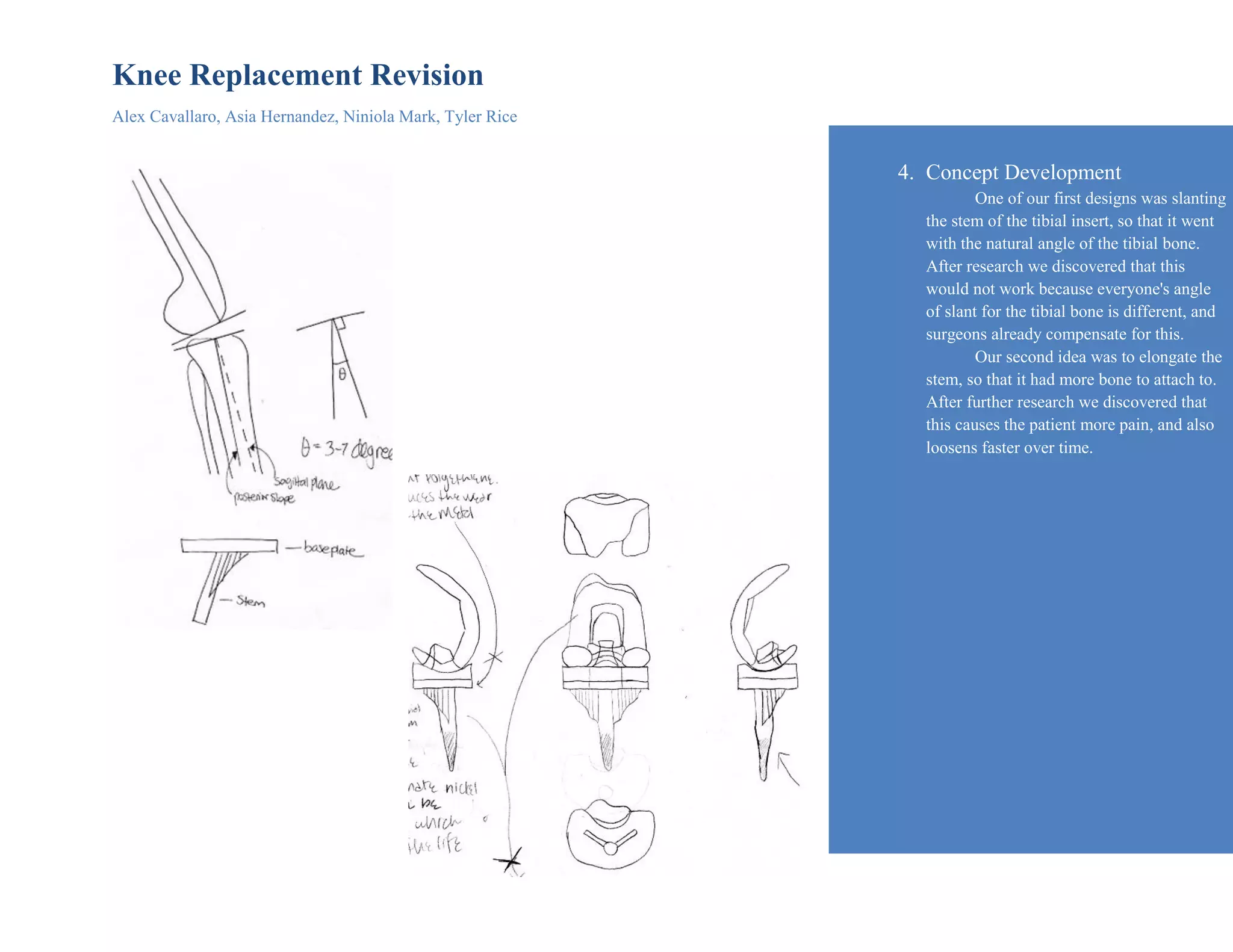
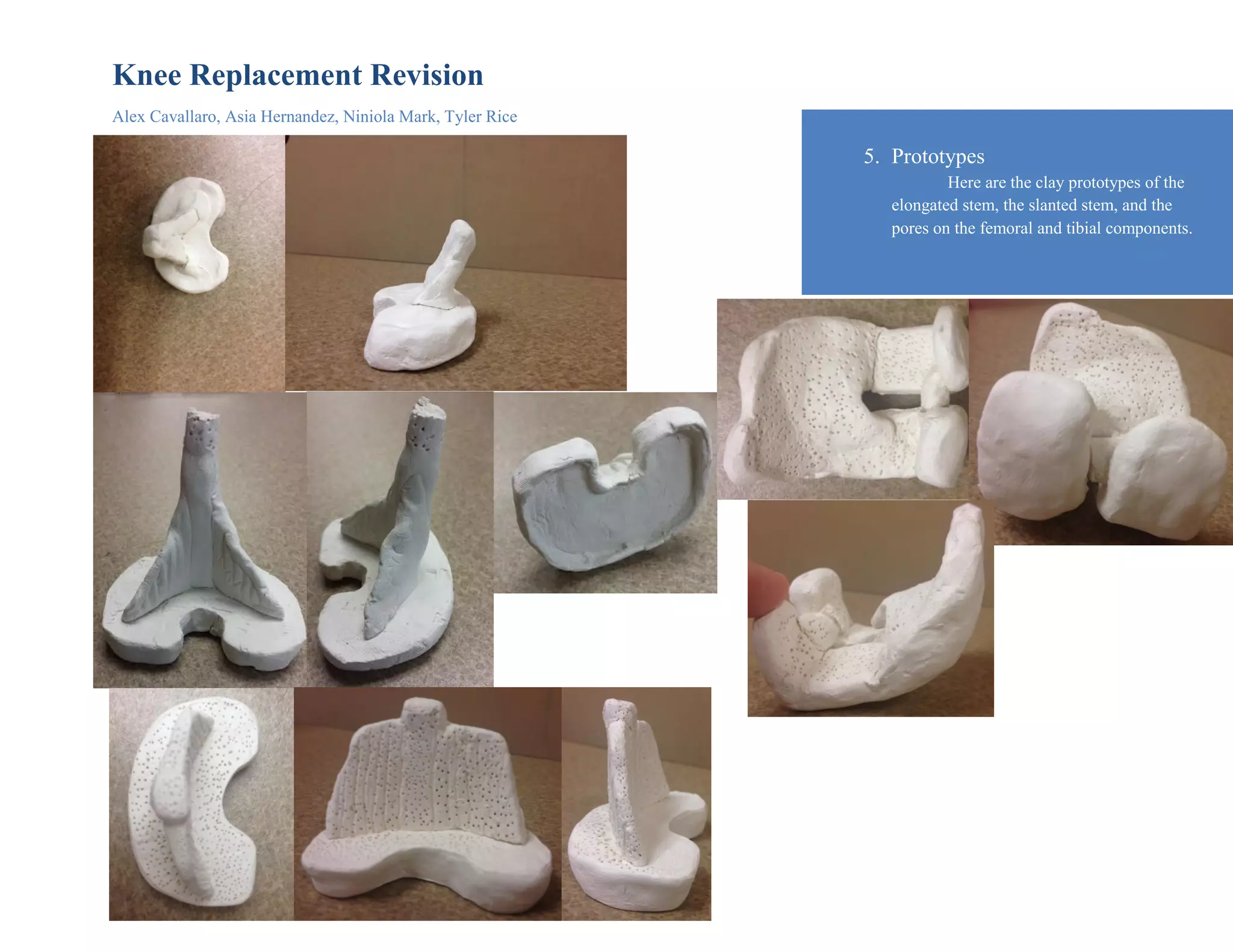
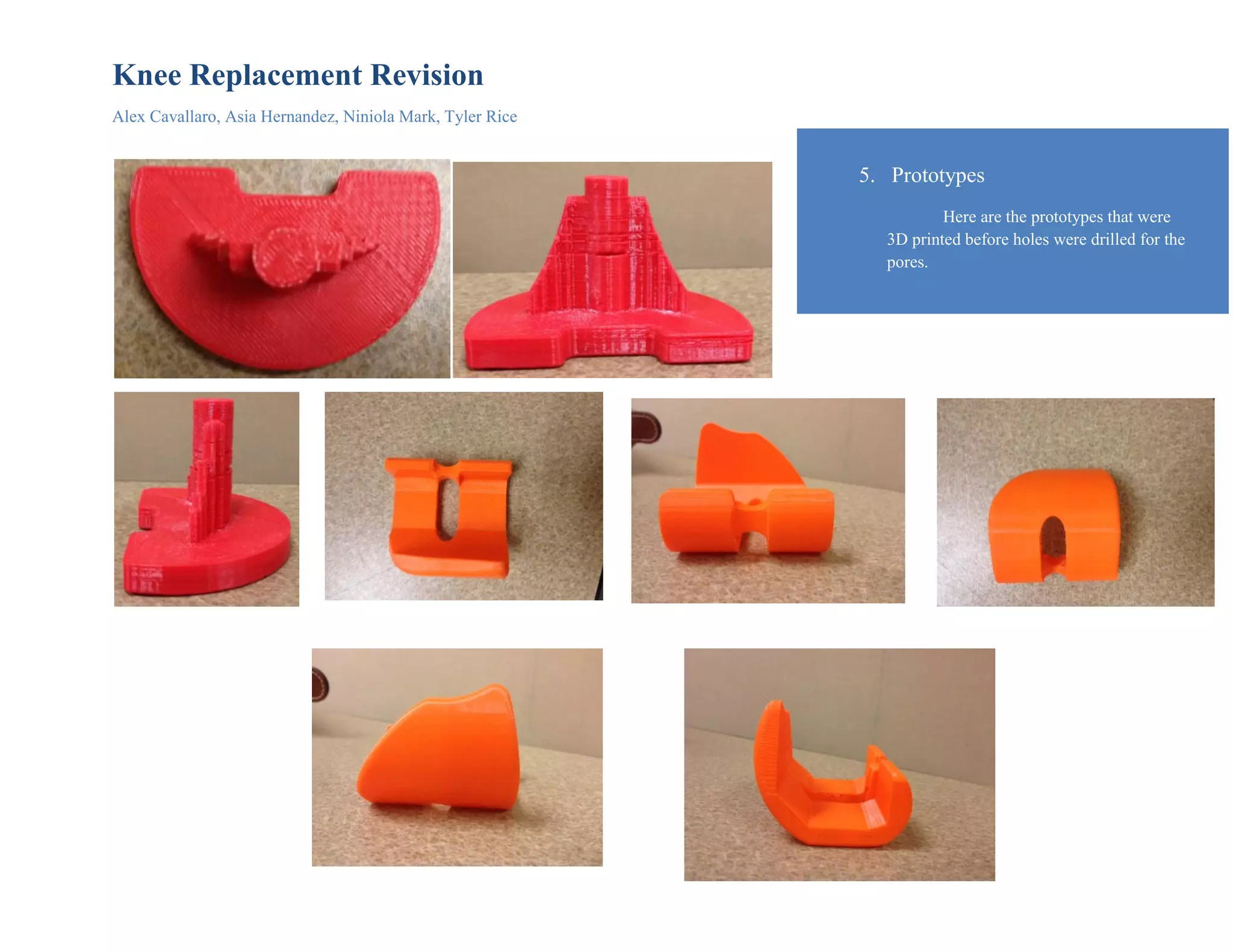
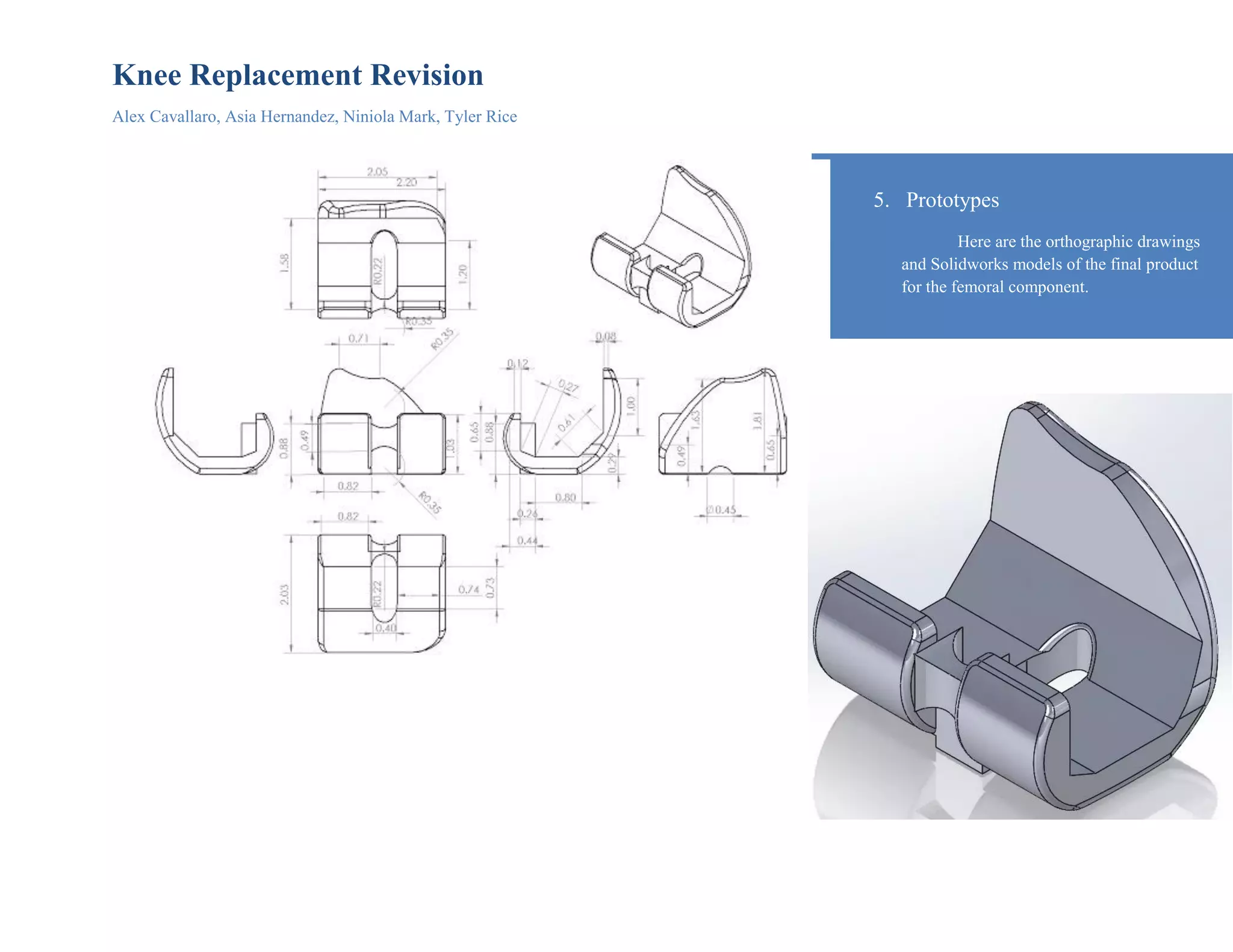
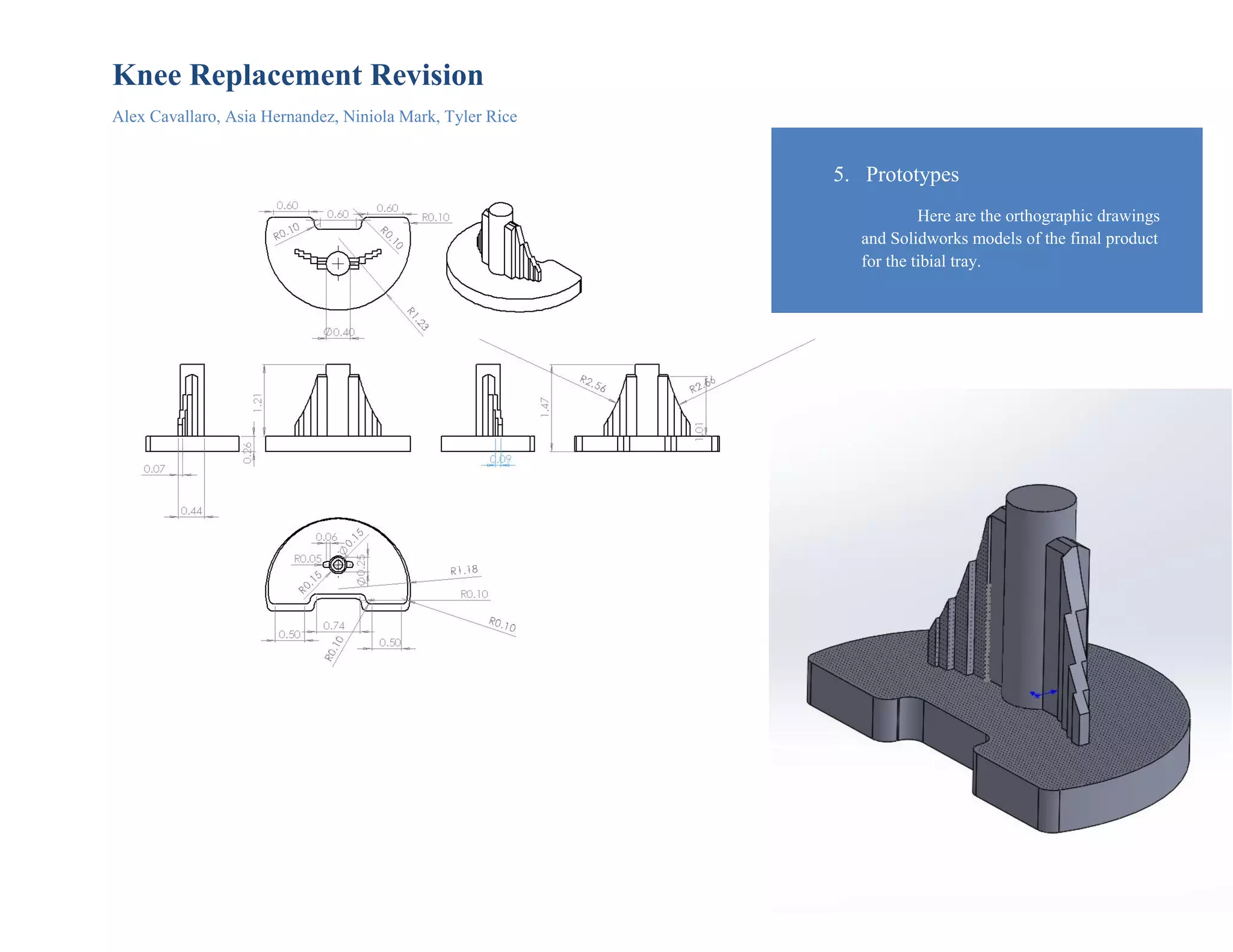
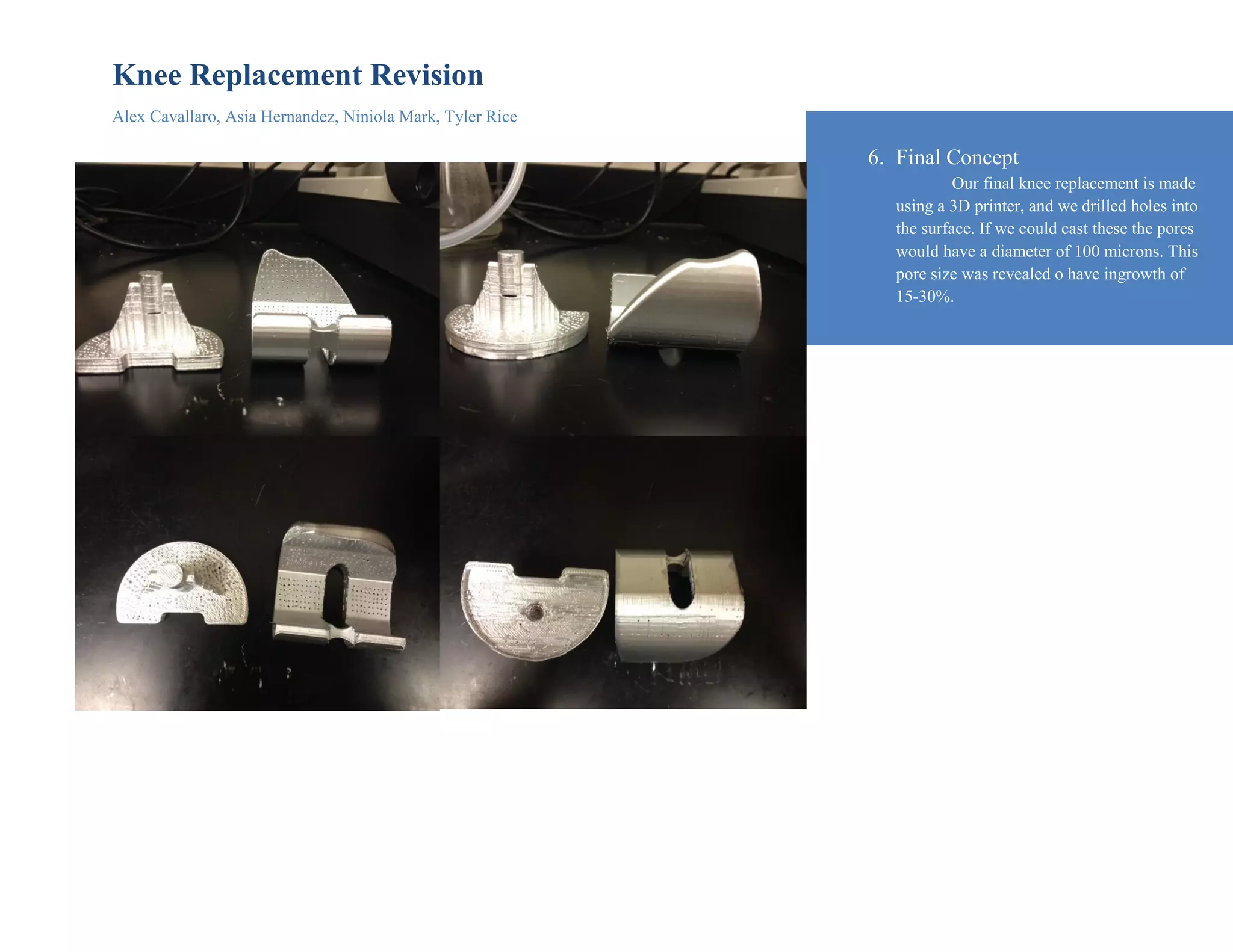
The document discusses a redesign of the Stryker Scorpio knee replacement system to last longer before revision surgery is needed. The target users are young, active patients aged 60 and younger. Through interviews, it was found that poor bone-implant fixation was a common cause of revision. The redesign uses titanium alloy components with a porous surface to encourage bone growth and improve fixation. Prototypes were created through 3D printing and drawings. The final concept adds pores of 100 microns, which research showed could increase bone ingrowth by 15-30%. This design aims to better suit active lifestyles and require fewer revision surgeries.