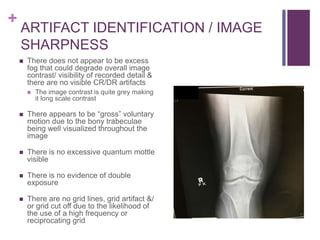
This document evaluates an AP knee x-ray image for quality, positioning, and compliance with standards. It finds that the image meets acceptance criteria overall but could be improved by better centering and removing artifacts. While diagnostic, the striped pattern over the distal femur should be identified and avoided in future images. Proper positioning and technique were utilized, though the contrast appears more grey than black and white as preferred.