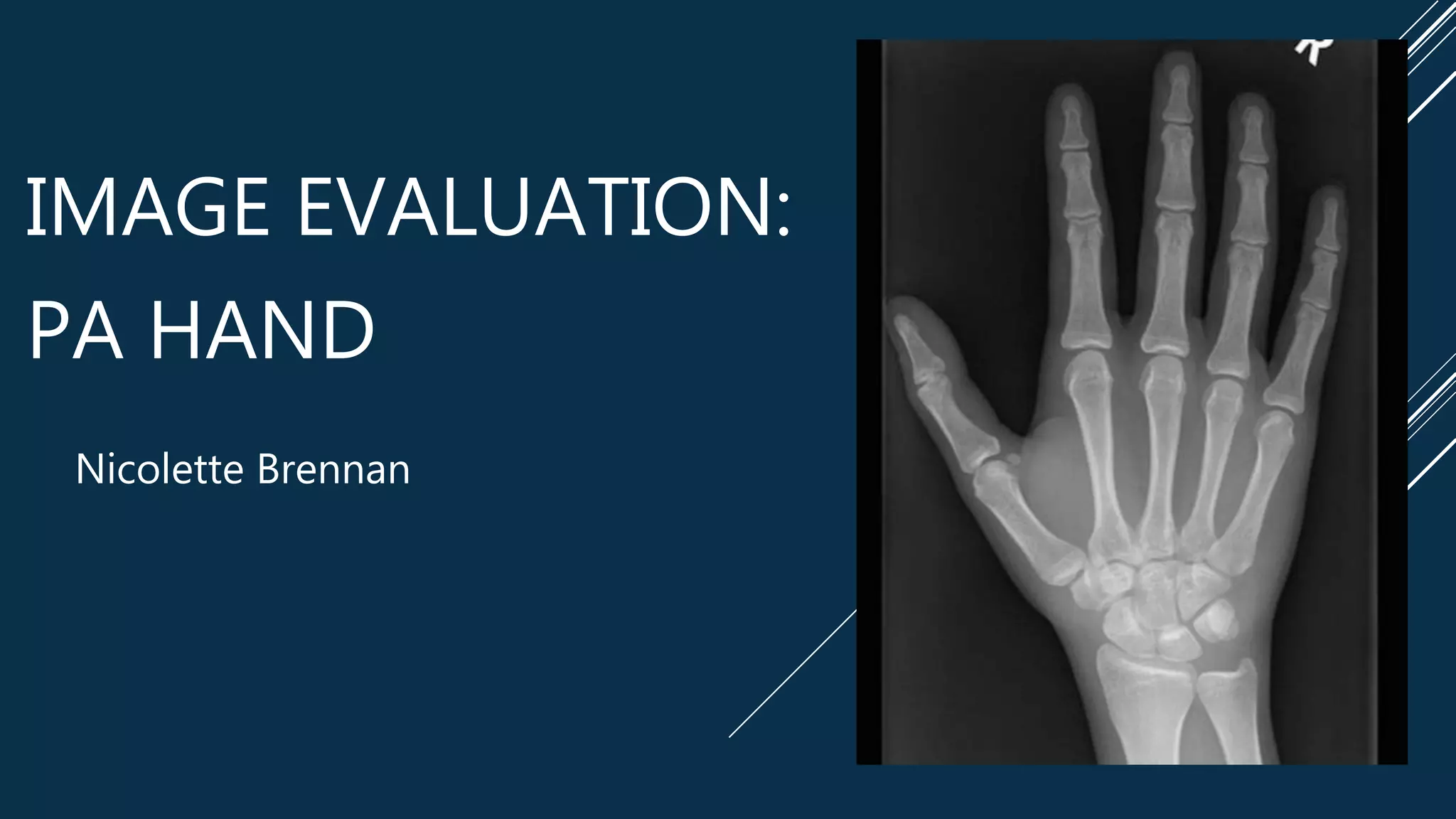
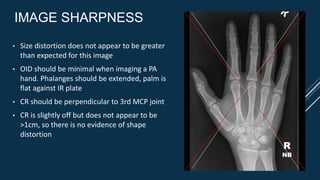
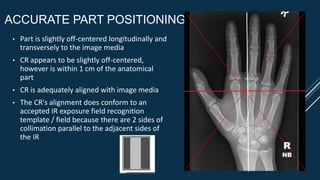
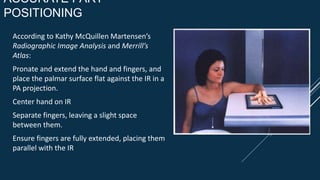
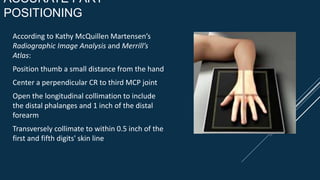
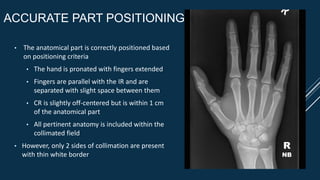
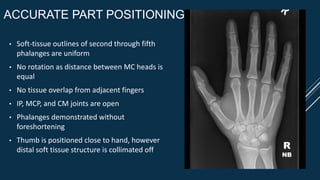
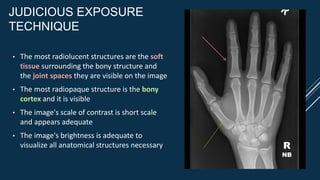
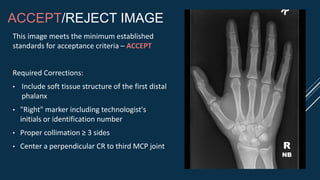
This image evaluation provides a detailed analysis of a PA hand x-ray image based on standards of HIPAA compliance, marker and patient identification, radiation hygiene, completeness of positioning/projection, artifact identification, image sharpness, accurate part positioning, and judicious exposure technique. While meeting minimum acceptance criteria, the summary identifies areas for improvement, including inclusion of soft tissue, proper marker and technologist identification, collimation on three sides, and centering of the CR. The evaluator recommends accepting the image with corrections.