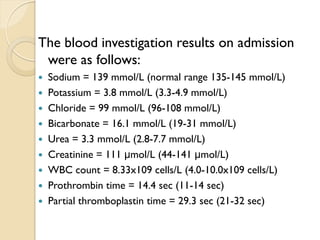
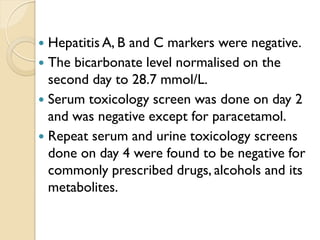
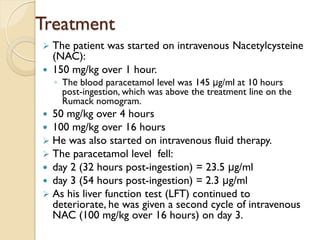
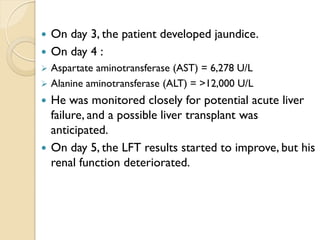
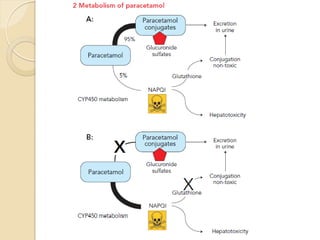
This case report discusses a 29-year-old man who experienced nephrotoxicity following a 30 g paracetamol overdose, presenting 10 hours post-ingestion with elevated liver enzymes and renal function issues. He was treated with intravenous N-acetylcysteine, which may have mitigated liver failure and reduced nephrotoxic severity. The report highlights that nephrotoxicity can occur independently of hepatotoxicity, emphasizing the need for further studies on risk factors and renal monitoring in paracetamol overdose cases.