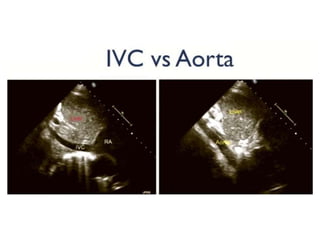
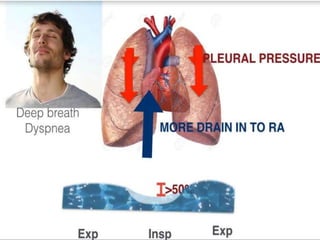
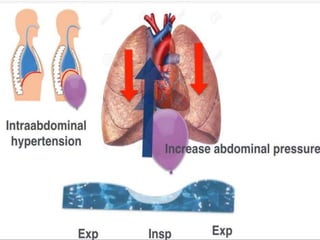
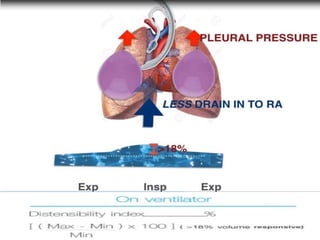
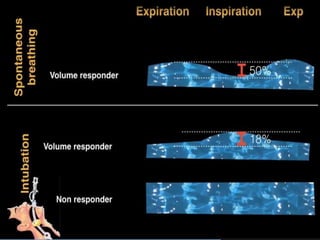
1) The document discusses using ultrasound measurement of the inferior vena cava (IVC) diameter to assess volume status in patients.
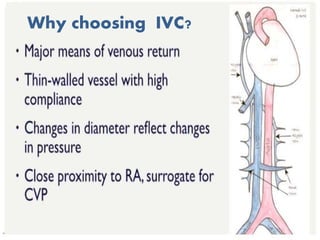
2) Measuring the IVC is a fast, reliable, and non-invasive method to detect volume status changes compared to other methods like central venous pressure measurement.
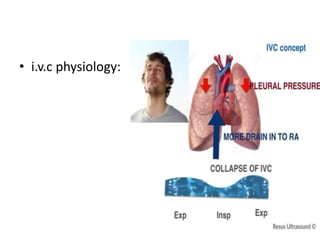
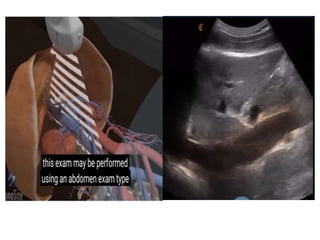
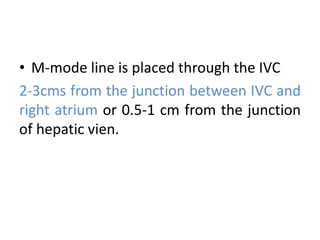
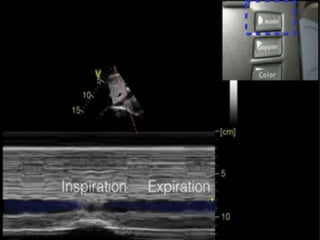
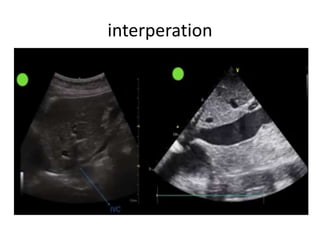
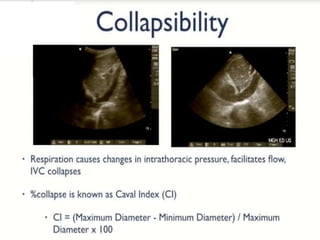
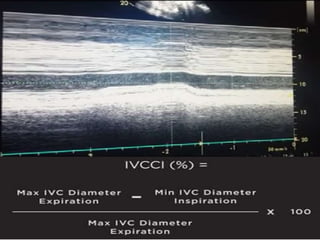
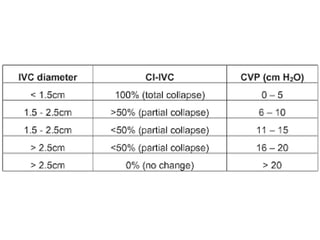
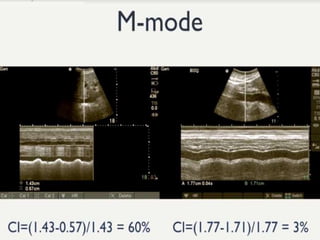
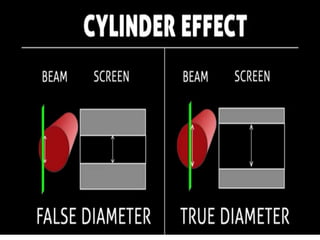
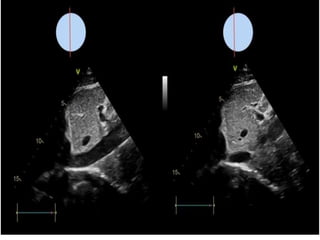
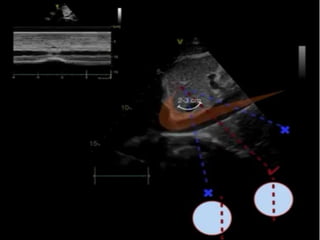
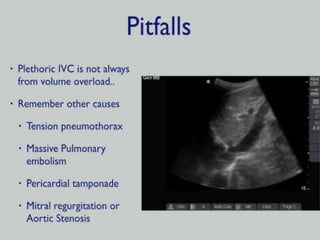
3) The document reviews the technique for measuring IVC diameter using ultrasound and interpreting the results to help guide clinical decisions like fluid administration in patients with abnormal volume status.