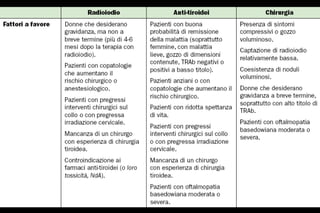
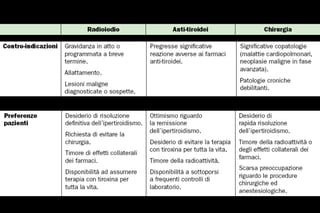
This document discusses definitive treatment options for Graves' disease. Radioactive iodine therapy is recommended in most cases as it is cost-effective and results in definitive hyperthyroidism cure by inducing hypothyroidism. Surgery is an alternative if the goiter is large or there is suspicion of thyroid cancer. The risks and benefits of radioactive iodine versus surgery should be considered based on each patient's individual circumstances and preferences.













































![Thyroid carcinoma final [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidcarcinomafinalpart2-161126043433-thumbnail.jpg?width=640&height=640&fit=bounds)































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










