Downloaded 42 times







![Dr. Mark Tulchinsky (2017 SNMMI
Annual meeting)
6/13/2017
CE88: Radioiodine Therapy for
Hyperthyroidism: The State of the Art 12
2015 ATA Guidelines
• 133 pages document
• Reviewed 1078 references, grading of the
evidence qualitatively
good, moderate, weak
• Made 101 recommendations, using
modified ACP system
strong, weak, no recommendation
• There is a broad range of new or modified
recommendations
21 were diametrically changed from 2009
• 133 pages document
• Reviewed 1078 references, grading of the
evidence qualitatively
good, moderate, weak
• Made 101 recommendations, using
modified ACP system
strong, weak, no recommendation
• There is a broad range of new or modified
recommendations
21 were diametrically changed from 2009
Abbreviations: ACP = American College of Physicians
Stated Aim versus Recommendation
Haugen BR et al. 2015 ATA guidelines. Thyroid
DOI: 10.1089/thy.2015.0020
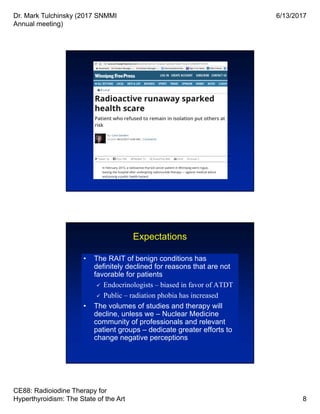
• AIM: “A major goal of these guidelines is to
minimize potential harm from overtreatment in
a majority of patients at low risk for disease-
specific mortality and morbidity, while
appropriately treating and monitoring those
patients at higher risk.” [AJCC/UICC staging?]
• RECOMMENDATION 48: “The 2009 ATA Initial
Risk Stratification System is recommended for
DTC patients treated with thyroidectomy, based
on its utility in predicting risk of disease
recurrence and/or persistence.”
• AIM: “A major goal of these guidelines is to
minimize potential harm from overtreatment in
a majority of patients at low risk for disease-
specific mortality and morbidity, while
appropriately treating and monitoring those
patients at higher risk.” [AJCC/UICC staging?]
• RECOMMENDATION 48: “The 2009 ATA Initial
Risk Stratification System is recommended for
DTC patients treated with thyroidectomy, based
on its utility in predicting risk of disease
recurrence and/or persistence.”](https://image.slidesharecdn.com/ts05radionuclidetherapybasicsfinalhandout-170622024005/85/I-131-Therapy-Current-Practice-and-Updates-12-320.jpg)





![Dr. Mark Tulchinsky (2017 SNMMI
Annual meeting)
6/13/2017
CE88: Radioiodine Therapy for
Hyperthyroidism: The State of the Art 22
• Drastic reductions in RAI pre-Rx scans & Rx
• Poor prep (rhTSH for stimulation, ±LID) =
poor scan (if done) = poor RAI Rx
• Authorized users responsible mostly for
dispensing RAI, if and when it’s ordered
• It may save $ for 3rd party payers … but at
what (or whose)?
• Drastic reductions in RAI pre-Rx scans & Rx
• Poor prep (rhTSH for stimulation, ±LID) =
poor scan (if done) = poor RAI Rx
• Authorized users responsible mostly for
dispensing RAI, if and when it’s ordered
• It may save $ for 3rd party payers … but at
what (or whose)?
The Good
“You can always count on Americans [American
Thyroid Association] to do the right thing - after
they've tried everything else.” Winston Churchill
The End?
131I](https://image.slidesharecdn.com/ts05radionuclidetherapybasicsfinalhandout-170622024005/85/I-131-Therapy-Current-Practice-and-Updates-22-320.jpg)

Dr. Mark Tulchinsky presented on the state of radioiodine therapy (RAI) for hyperthyroidism at the 2017 SNMMI annual meeting, emphasizing the historical background, current practices, and evolving guidelines surrounding the treatment. He highlighted the risk of worsening Graves' orbitopathy associated with RAI and the decline in its use due to biases and public fear of radiation. Additionally, the presentation discussed the importance of imaging and evidence-based approaches in managing thyroid conditions and related therapies.



































































