Download as PDF, PPTX







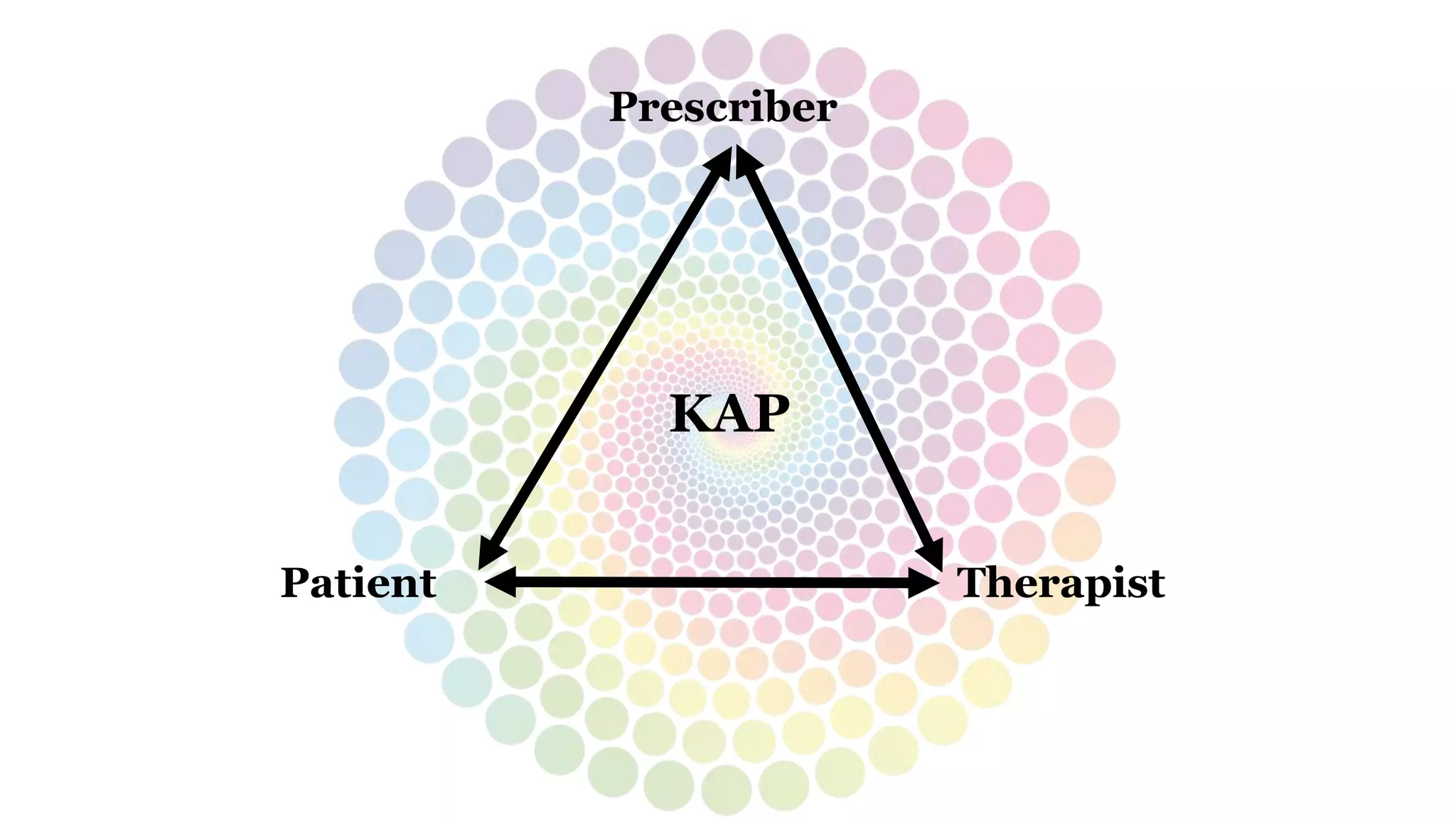












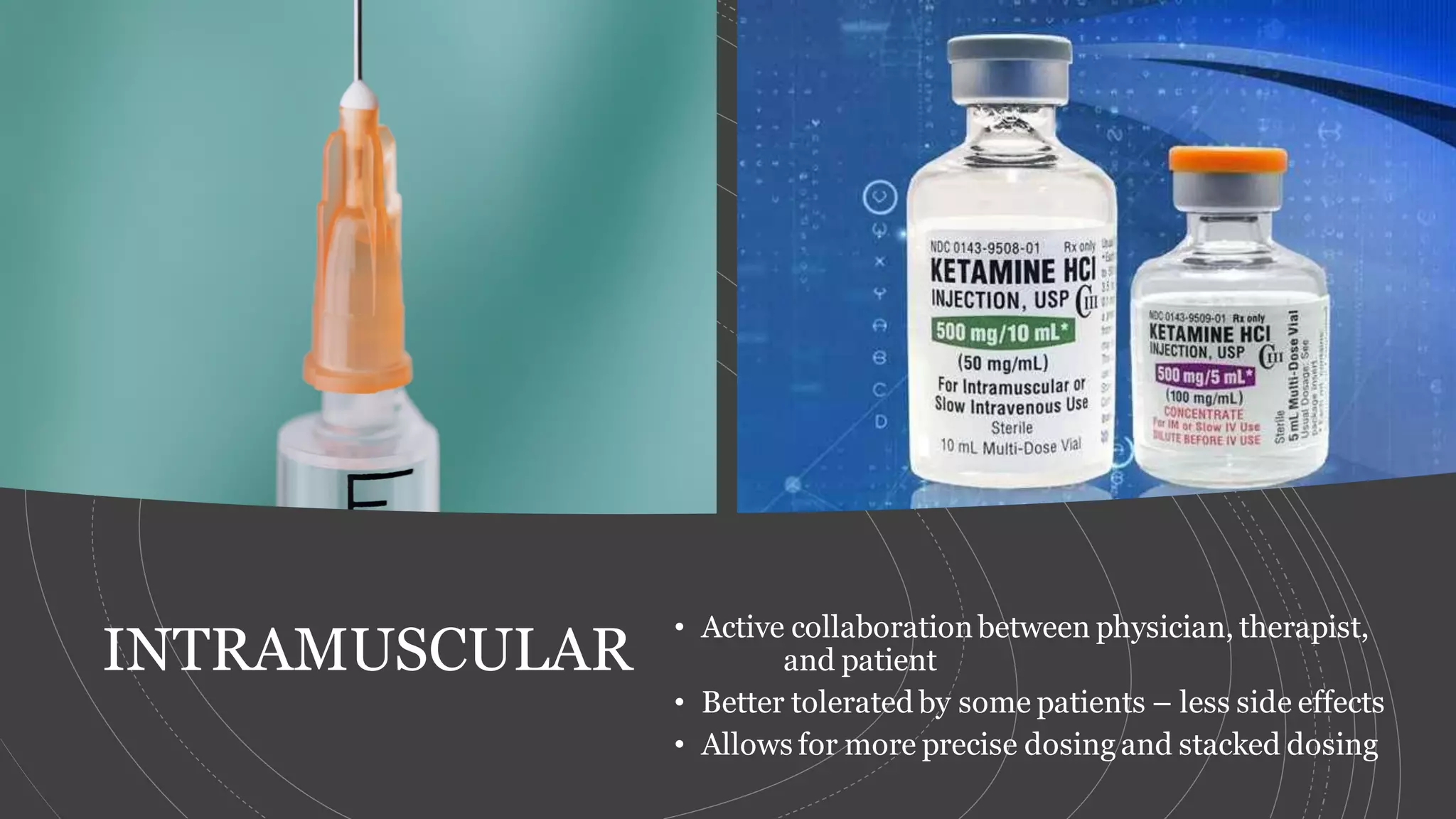
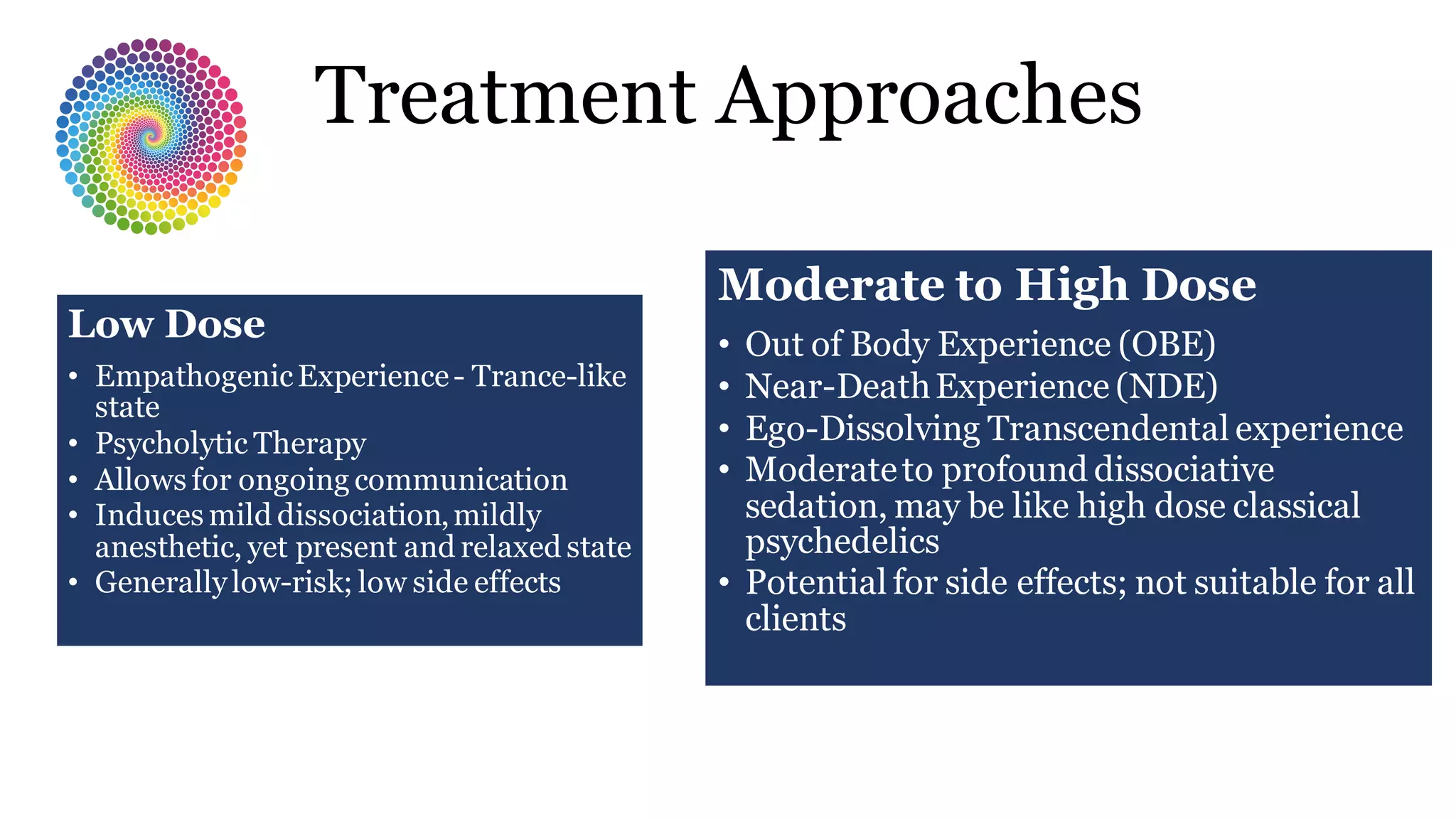









This document provides an overview of ketamine-assisted psychotherapy (KAP). It discusses ketamine's rapid onset and safety profile, and its ability to access different states of consciousness for therapeutic purposes. Key aspects of the KAP process are outlined, including medical intake and screening, psychological preparation, low to high dosing strategies, and potential experiences during sessions like empathogenic states. Risks and challenges of KAP are addressed. Major goals of the integration process after sessions are described, such as emotional processing and resolving pathogenic beliefs. The document promotes a multidisciplinary treatment approach and lists training opportunities provided by Polaris Insight Center.


































































