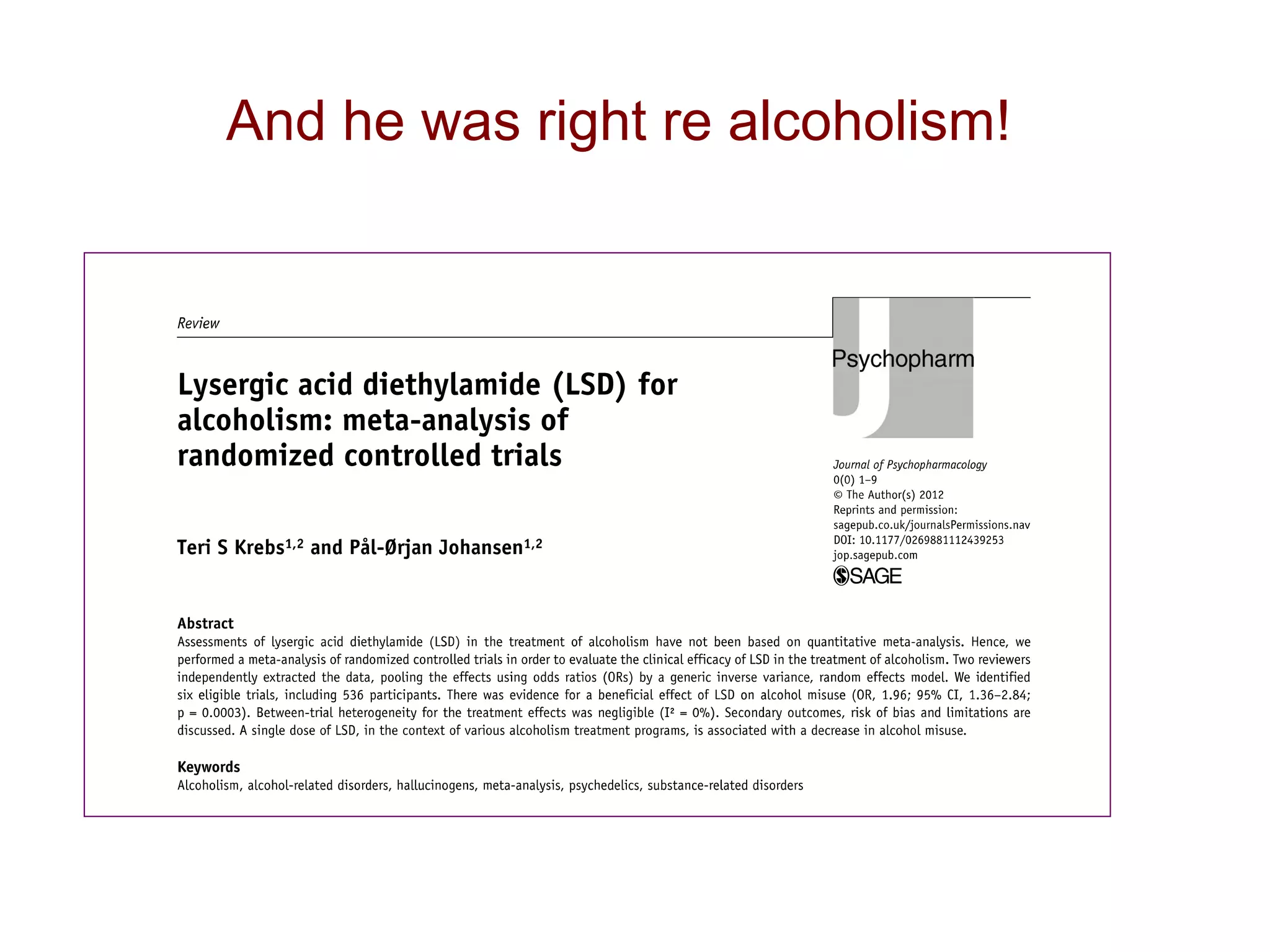
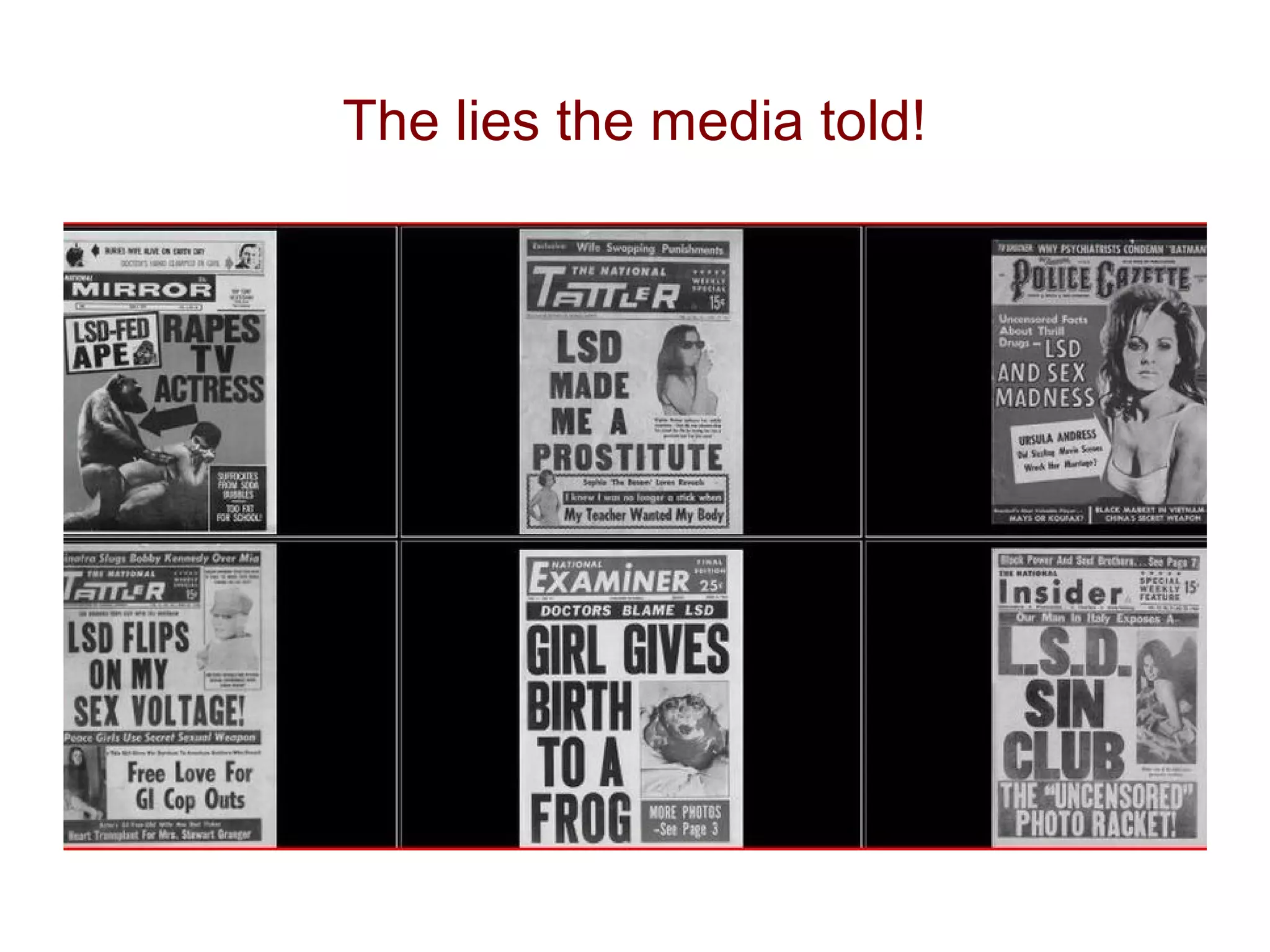
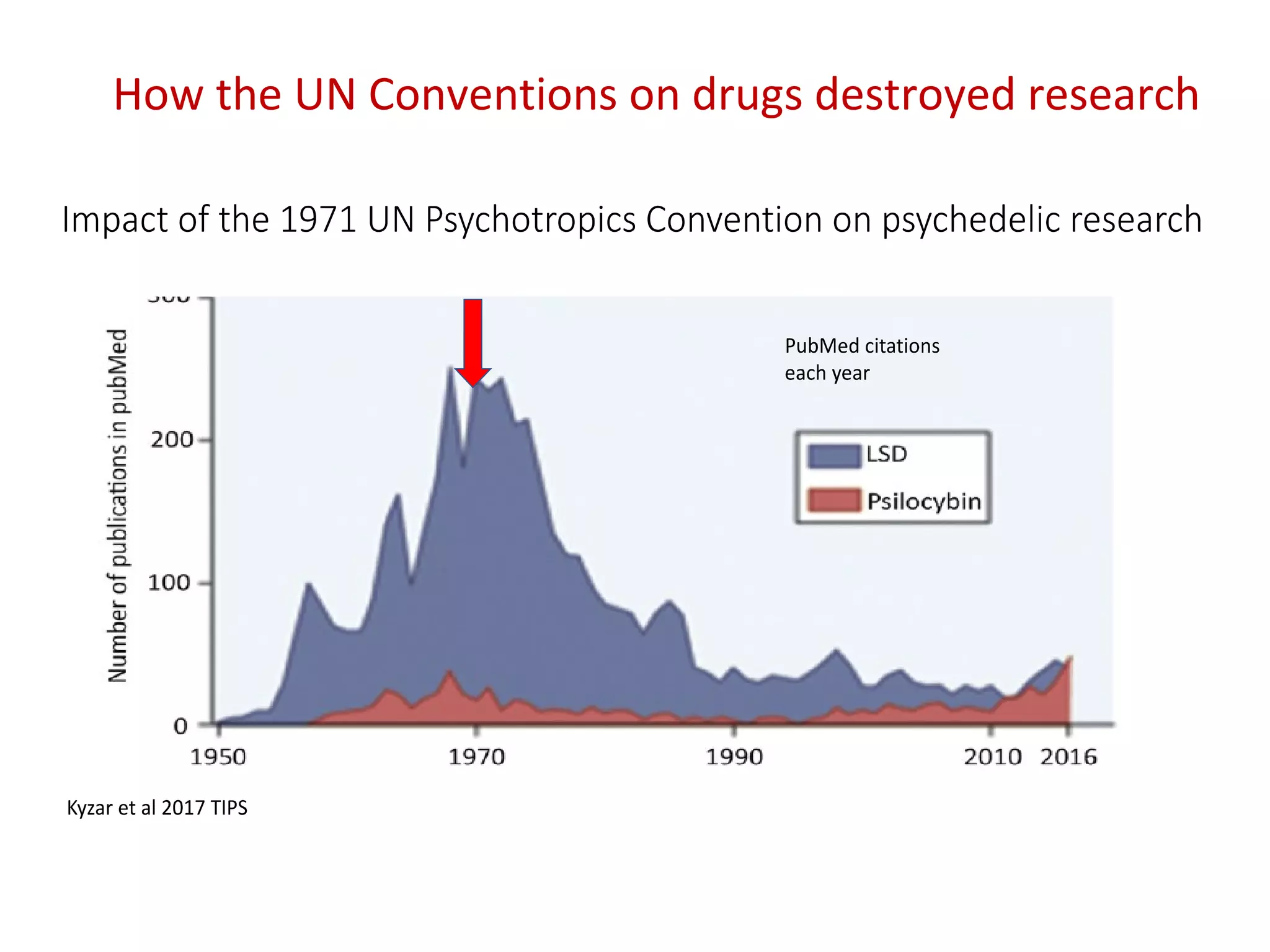
The document summarizes research on psychedelic-assisted psychotherapy. It discusses how psychedelics like LSD, psilocybin, and ketamine were widely used in psychotherapy in the 1950s and 1960s to treat addiction and depression, with largely positive results. However, psychedelics were banned in the 1970s. Recent research has started exploring psychedelic-assisted psychotherapy again. Studies discussed show psilocybin-assisted therapy helped alcoholics stay sober and helped smokers quit. Ketamine therapy was more effective for treating heroin addiction with multiple sessions compared to a single session. The document also reviews neuroscience research on how psychedelics affect brain activity and connectivity, particularly reducing activity in regions linked to depression.







![LSD and all other psychedelics banned in
face of opposition from senators
Bobby Kennedy:
Why if [clinical LSD projects] were worthwhile
six months ago, why aren’t they worthwhile
now? . . . We keep going around and
around. . . . If I could get a flat answer about
that I would be happy. Is there a
misunderstanding about my question?
I think perhaps we have lost sight of the
fact that LSD can be very, very helpful in
our society if used properly.”
quoted in Lee & Shlain, 1985, p. 93)
Has there ever been a worst example of research
censorship?
Well not since …….](https://image.slidesharecdn.com/davidnutt-180706131658/75/PROFESSOR-DAVID-NUTT-PSYCHEDELIC-ASSISTED-PSYCHOTHERAPY-NEW-NEUROSCIENTIFIC-APPROACHES-TO-ADDICTION-AND-DEPRESSION-19-2048.jpg)









![PET image
[11C]Cimbi-36
5HT2A receptor
agonist
Copenhagen
5HT2A receptors most densely expressed cortex
Human brain has highest density of any brain
The 5-HT2A receptor in human brain revealed by
PET](https://image.slidesharecdn.com/davidnutt-180706131658/75/PROFESSOR-DAVID-NUTT-PSYCHEDELIC-ASSISTED-PSYCHOTHERAPY-NEW-NEUROSCIENTIFIC-APPROACHES-TO-ADDICTION-AND-DEPRESSION-32-2048.jpg)








![Psilocybin changes attitude
They can change patients’ outlook
Normalised
post-treatment
P < 0.01
P < 0.01
Pessimism bias
pre-treatment
P < 0.01
“My outlook has changed significantly. I'm more aware now that it's
pointless to get wrapped up in endless negativity. I feel as if I've
seen a much clearer picture.”
[Patient from depression trial, male, aged 52, >20yrs depression]
Watts et al Journal of Humanistic Psychology 2017, Vol. 57(5) 520](https://image.slidesharecdn.com/davidnutt-180706131658/75/PROFESSOR-DAVID-NUTT-PSYCHEDELIC-ASSISTED-PSYCHOTHERAPY-NEW-NEUROSCIENTIFIC-APPROACHES-TO-ADDICTION-AND-DEPRESSION-52-2048.jpg)
![It was like when you defrag the hard drive on your
computer, I experienced blocks going into place, things being
rearranged in my mind, I visualized as it was all put into
order, a beautiful experience with these gold blocks going
into black drawers that would illuminate, and I thought my
brain is bring defragged, how brilliant is that! (P11)
My mind works differently [now]. I ruminate much
less, and my thoughts feel ordered, contextualized.
Rumination was like thoughts out of context, out of
time; now my thoughts feel like they make sense,
with context and logical flow. (P11) “
“
Another quote
Watts et al Journal of Humanistic Psychology 2017, Vol. 57(5) 520](https://image.slidesharecdn.com/davidnutt-180706131658/75/PROFESSOR-DAVID-NUTT-PSYCHEDELIC-ASSISTED-PSYCHOTHERAPY-NEW-NEUROSCIENTIFIC-APPROACHES-TO-ADDICTION-AND-DEPRESSION-53-2048.jpg)


![Talking therapy: disconnection:
I’m sick to the back teeth of telling people again and again the backstory.
All the talking therapies, each time you go for an 8 or 6 week course of
that stuff, you spend the first few weeks going over the stuff, they ask all
the questions again then its session 4, and then, you think who’s learning
something here, ‘cos I’m not. You are! (P13)
They all seemed to be trying to fit a person into a preconceived set of
patterns: ‘try to do this’, ‘make this your goal, and we’ll measure it’. But
just having these goals set for you is more pressure and when you don’t
meet those goals, you feel even worse because you’re letting them down,
and you already feel let down yourself! (P1)
TOO DIRECTIVE
TOO SHORT
“
“
I got up the courage to tell him, I’d never told anyone. And [the
psychiatrist] just looked at his shoes.’ (P16)
DON’T ADDRESS TRAUMA:
“](https://image.slidesharecdn.com/davidnutt-180706131658/75/PROFESSOR-DAVID-NUTT-PSYCHEDELIC-ASSISTED-PSYCHOTHERAPY-NEW-NEUROSCIENTIFIC-APPROACHES-TO-ADDICTION-AND-DEPRESSION-56-2048.jpg)


































































































