Download as PDF, PPTX

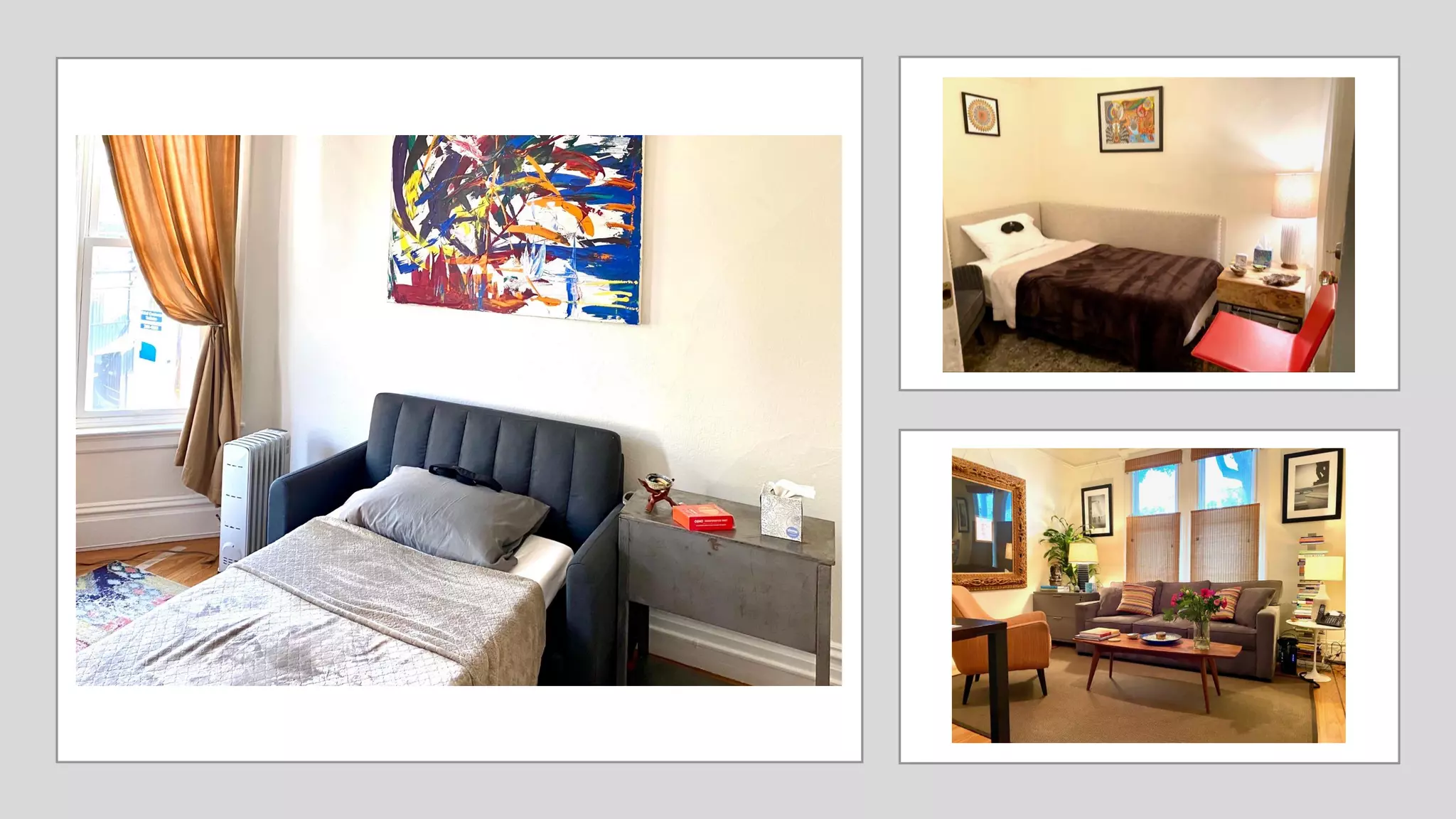









This document provides an overview of ketamine-assisted psychotherapy training at Polaris Insight Center. It discusses ethical considerations for ketamine therapy including codes of ethics, the importance of set and setting, preventing misconduct, and ensuring access. It also covers conducting group ketamine sessions, virtual ketamine therapy, integrating spiritual experiences, and future training opportunities.































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



