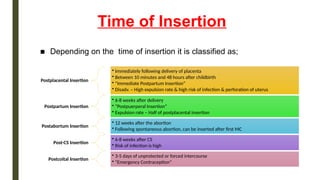
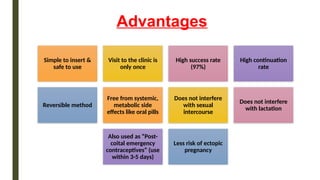
The document provides an overview of intrauterine contraceptive devices (IUDs), detailing their history, types (first, second, and third generation), mechanisms of action, ideal candidates, insertion timings, and post-insertion advice. It highlights the advantages such as high success rates and reversibility, as well as disadvantages including potential menstrual changes and risk of pelvic infection. Overall, it serves as a comprehensive guide on the use, effectiveness, and considerations regarding IUDs in contraception.













































![GROUP FOUR REPRODUCTIVE HEALTH PRESENTATION_ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/groupfourreproductivehealthpresentationppt1-240318002334-7df02886-thumbnail.jpg?width=640&height=640&fit=bounds)

































