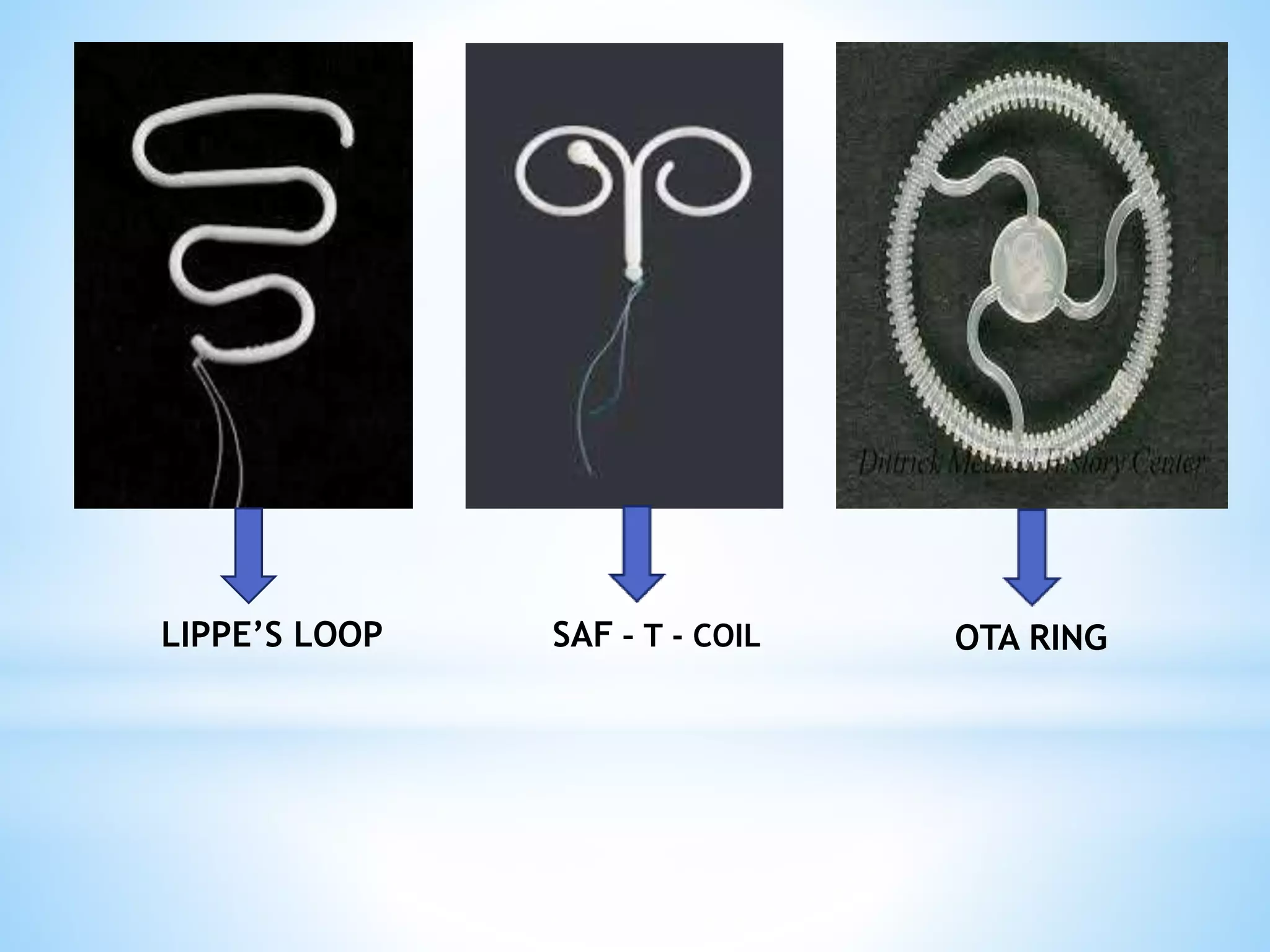
IUCDs are long-term, reversible contraceptive devices that are placed inside the uterus. There are three generations of IUCDs - first generation contain inert materials, second generation contain copper, and third generation release hormones like progesterone. Copper IUCDs work by creating inflammation and altering the uterine environment, while hormone-releasing IUCDs thin the endometrium and alter cervical mucus. IUCDs are effective for 3 to 10 years depending on the specific device. Complications can include pain, bleeding, and rarely perforation or ectopic pregnancy. Pregnancy with an IUCD carries additional risks. Newer frameless and Essure devices aim to reduce side effects.



























































![GROUP FOUR REPRODUCTIVE HEALTH PRESENTATION_ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/groupfourreproductivehealthpresentationppt1-240318002334-7df02886-thumbnail.jpg?width=640&height=640&fit=bounds)




















