Download to read offline

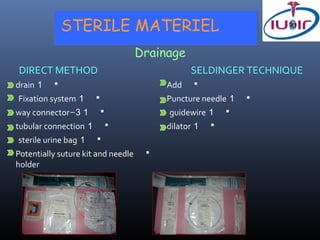
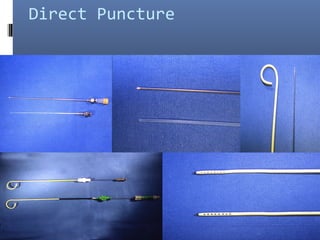


The document discusses biopsy and drainage procedures. It provides details on: 1) Biopsy results being positive 70-100% of the time, with the lowest success for lymphoma. 2) Techniques for abdominal drainage including direct puncture and the Seldinger technique using various sterile materials. 3) Precautions for drainage including using a fine needle to determine fluid characteristics and never fully emptying before draining.






















































































