Interstitial Cystitis - PPT.pptx AND ITS TREATMENT
1.
CBDC 2ND
BHMS COURSE
DAY- FRIDAY
DATE - 18/10/2024
TOPIC - Interstitial Cystitis
PRESENTED BY - DR. MRS. M. A. NERLEKAR
2.
Definition
● Interstitial cystitis(i.e., chronic pelvic pain syndrome) is a
persistent, painful form of chronic cystitis occurring most
frequently in women. It is characterized by intermittent,
often severe suprapubic pain, urinary frequency, urgency,
hematuria and dysuria without evidence of bacterial
infection,
● The AUA guideline defines IC/BPS as "an unpleasant
sensation (pain, pressure, discomfort) perceived to be
associated with the urinary bladder, accompanied by lower
urinary tract symptoms of more than 6 weeks duration, in
the absence of infection or other identifiable causes." IC
has classically been used to describe the clinical syndrome
of urgency/frequency and pain in the bladder and/or
pelvic area.
3.
Etiology
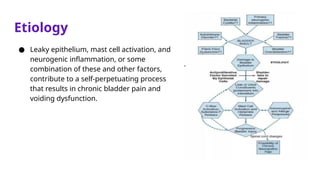
● Leaky epithelium,mast cell activation, and
neurogenic inflammation, or some
combination of these and other factors,
contribute to a self-perpetuating process
that results in chronic bladder pain and
voiding dysfunction.
4.
Etiology
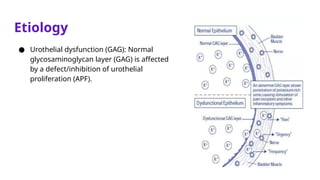
● Urothelial dysfunction(GAG): Normal
glycosaminoglycan layer (GAG) is affected
by a defect/inhibition of urothelial
proliferation (APF).
5.
Clinical Presentation
● PAIN:Suprapubic or pelvic discomfort
● Bladder pain that intensifies with bladder
filling and is relieved by voiding
● Dysuria
● Urinary frequency and urgency
● Nocturia: mild to severe (1 to more than 12
times per night)
● Spasms of the rectum and levator ani
muscles
● Tenderness in the anterior vaginal wall,
suprapubic area, and pelvic floor muscles
during pelvic examination
● Women:
- Dysfunction
- Dyspareunia
- Female sexual discomfort
● Men:
- Pain at the tip of the penis, in
the groin, or in the testes
- Ejaculation frequently causes
pain due to significant pelvic
floor spasms
- Tenderness in the prostate,
bladder, testes, and epididymis
6.
Diagnosis
Inclusion Criteria
● Hunner’sulcers
● Glomerulations on
endoscopy
● Pain on bladder filling
relieved by emptying
● Pain (suprapubic,
perineal, pelvic,
urethral)
● Decreased bladder
compliance on
cystometrogram
Exclusion Criteria
● < 18 years
● Bladder tumors
● TB cyst
● Bacterial cystitis
● Gyn carcinomas
● Active herpes
● Bladder calculi
● Frequency < 5 in 12
hours
● Nocturia < 2
● Symptoms relieved
by antibiotics or
urine analgesics
● Bladder cap > 400
ML
● Duration < 12
months
7.
Diagnosis
Diagnostic Criteria forInterstitial Cystitis :
Category A: At least one of the following cystoscopic findings:
1. Diffuse glomerulations ( 20 per quadrant) in at least 3 quadrants of the
≥
bladder
2. A classic Hunner’s ulcer
Category B: At least one of the following symptoms:
3. Pain associated with the bladder
4. Urinary urgency
8.
Investigation
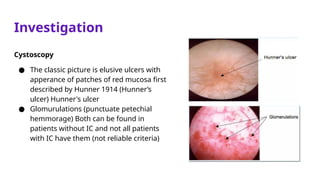
Cystoscopy
● The classicpicture is elusive ulcers with
apperance of patches of red mucosa first
described by Hunner 1914 (Hunner’s
ulcer) Hunner's ulcer
● Glomurulations (punctuate petechial
hemmorage) Both can be found in
patients without IC and not all patients
with IC have them (not reliable criteria)
9.
Investigation
Potassium Test
● Anintravesical potassium chloride challenge (KCI test) has been proposed
for diagnosis using a 0.4M potassium chloride solution Pain and
provocation of symptoms by potassium constitute a positive test.
10.
Treatment
● Conservative treatmentsfirst
○ Behavioral modification : control fluid intake , timed voiding , pelvic muscle
training
● Avoid surgery if possible
○ Exception is fulguration of Hunner’s lesions, must be done first
● Multiple simultaneous treatments often best
○ Pain management should be priority
References
● Robbins BasicPathology
● National Institute of Diabetes and Digestive and Kidney Diseases
● Hanno PM, Burks DA, Clemens JQ, Dmochowski RR, Erickson D, FitzGerald
MP, et al. AUA Guideline for the Diagnosis and Treatment of Interstitial
Cystitis/Bladder Pain Syndrome. Journal of Urology [Internet]. 2011 Jun 1
[cited 2024 Oct 17];185(6):2162–70. Available from:
https://doi.org/10.1016/j.juro.2011.03.064


![References
● Robbins Basic Pathology
● National Institute of Diabetes and Digestive and Kidney Diseases
● Hanno PM, Burks DA, Clemens JQ, Dmochowski RR, Erickson D, FitzGerald
MP, et al. AUA Guideline for the Diagnosis and Treatment of Interstitial
Cystitis/Bladder Pain Syndrome. Journal of Urology [Internet]. 2011 Jun 1
[cited 2024 Oct 17];185(6):2162–70. Available from:
https://doi.org/10.1016/j.juro.2011.03.064](https://image.slidesharecdn.com/interstitialcystitis-ppt-250519154419-42e5da44/85/Interstitial-Cystitis-PPT-pptx-AND-ITS-TREATMENT-13-320.jpg)



![Interstitial cystitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/interstitialcystitis1-150315053919-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)












































