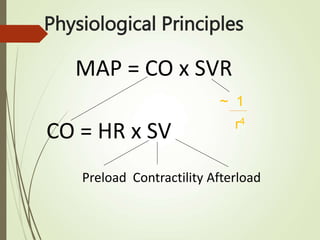
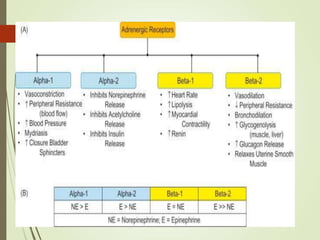
This document discusses inotropes and vasopressors used to treat shock. It defines inotropes as agents that increase myocardial contractility and cardiac index, while vasopressors increase vascular tone and elevate mean arterial pressure. The main types discussed are catecholamines like dopamine, dobutamine, adrenaline and norepinephrine. Phosphodiesterase inhibitors and vasopressin are also mentioned. Clinical indications, dosages, and hemodynamic effects are provided for various drugs. The goal of treatment is to perfuse tissues and oxygenate the body through managing preload, contractility, afterload and optimizing cardiac output and systemic vascular resistance. Early recognition and treatment of shock, along with