
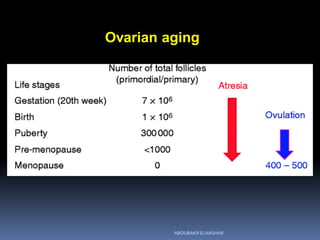
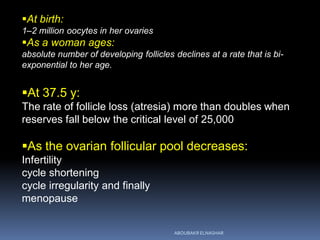
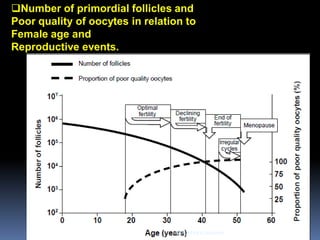
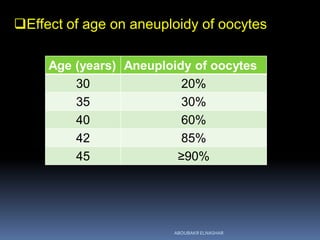

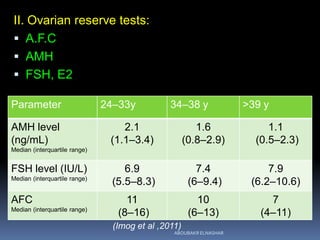

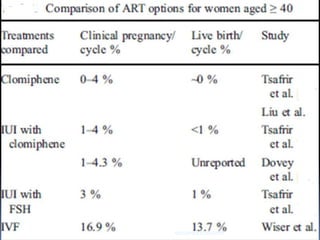
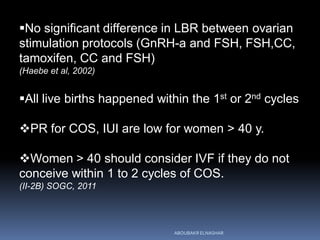
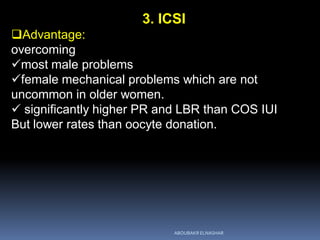
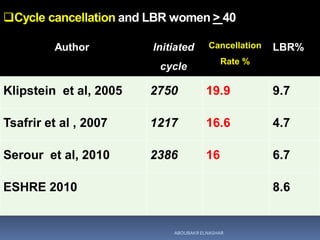
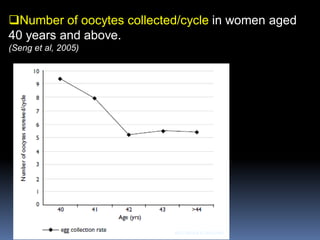
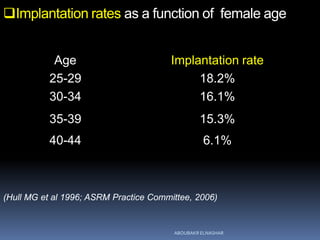
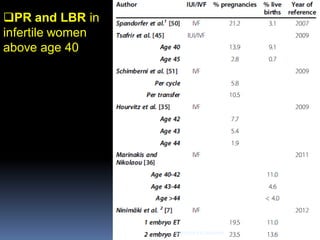


The document discusses infertility issues for women over 40. It notes that 15% of women now delay childbearing until after age 40. Ovarian aging leads to a decline in both egg quantity and quality with increasing female age. After age 40, evaluation should include tests of ovarian reserve like AMH, AFC, and FSH. IVF is the best treatment option for these women, though success rates decline sharply after age 43. Oocyte donation is the only effective treatment for infertility caused by declining egg quality due to age.

































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









