Downloaded 26 times

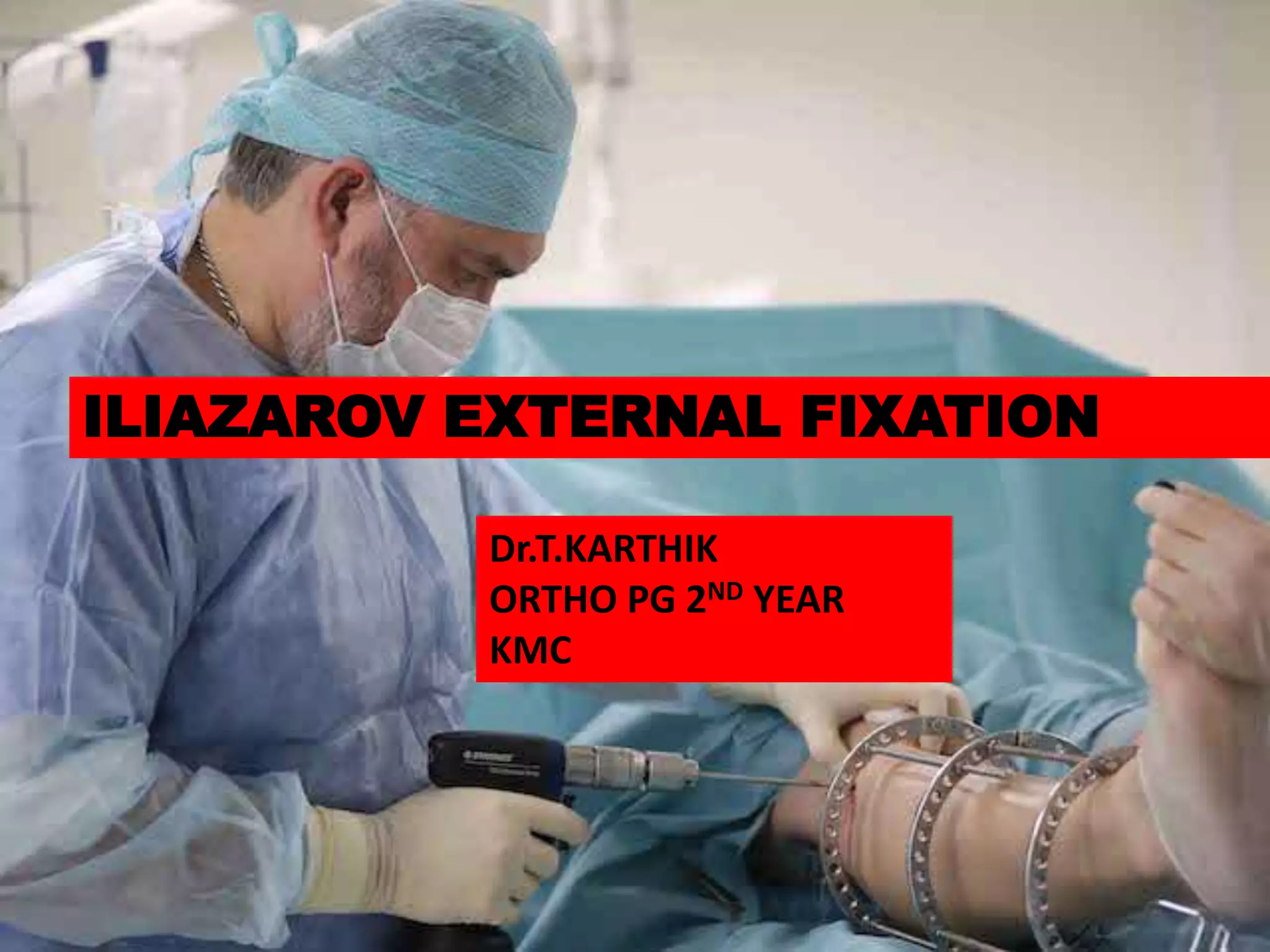









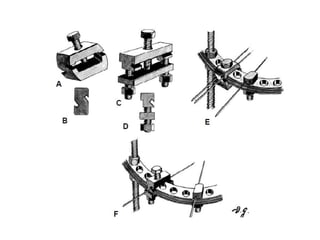

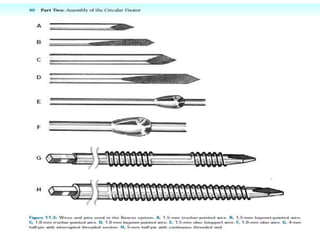
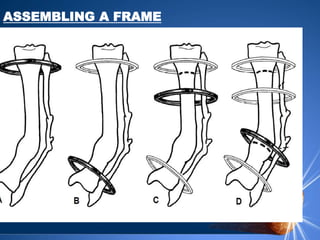
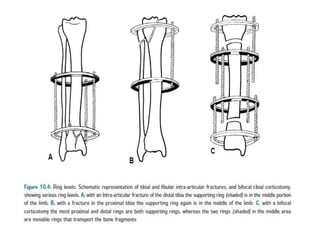

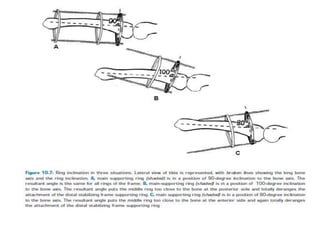

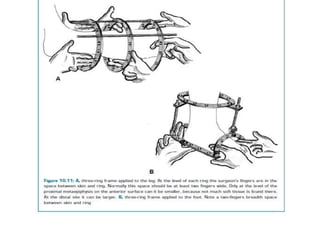


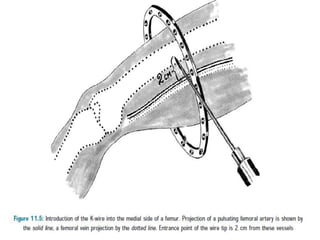












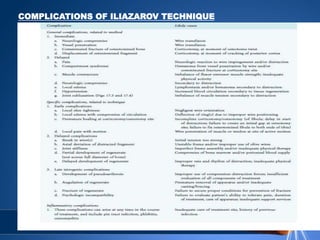


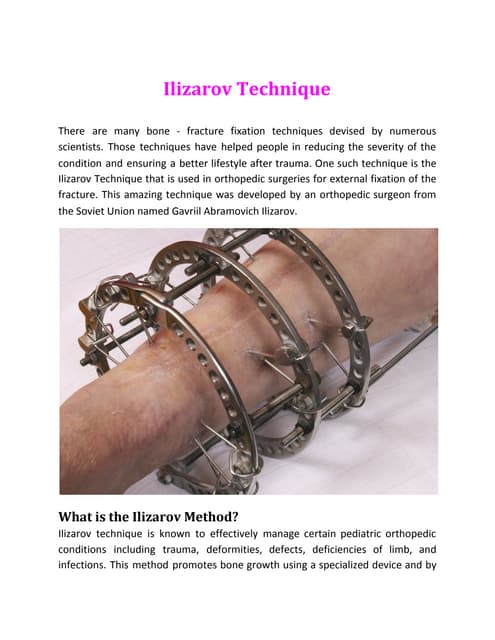
The document discusses the Ilizarov external fixation technique for bone lengthening and reconstruction. It covers the biomechanics and components of the Ilizarov frame, how to assemble it, and the application process including corticotomy, distraction, compression, and bone transport. Potential complications are addressed as well as frame removal. The Ilizarov technique uses gradual tension applied by an external fixator to regenerate bone and soft tissue through the biological process of distraction osteogenesis.