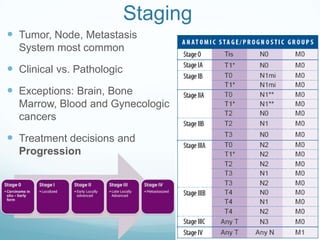
Staging
Tumor, Node,Metastasis
System most common
Clinical vs. Pathologic
Exceptions: Brain, Bone
Marrow, Blood and Gynecologic
cancers
Treatment decisions and
Progression
6.
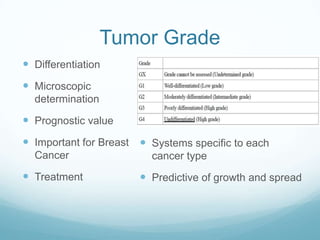
Tumor Grade
Differentiation
Microscopic
determination
Prognostic value
Important for Breast Systems specific to each
Cancer cancer type
Treatment Predictive of growth and spread
7.
Immune Score
NewConcept (Finalizes in December 2012)
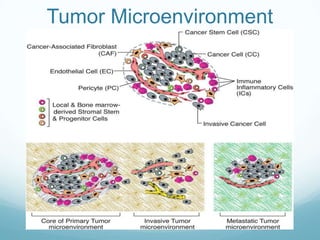
Incorporates Tumor Microenvironment
IHC to characterize tumor infiltrates for staging
Seeks to enhance prediction of prognosis and
response to treatment
Infiltrates – center of tumor, invasive margins, adjacent
lymphoid islets
Ultimate Goal: Density and location of immune cells
within tumor (influence survival/relapse risk)
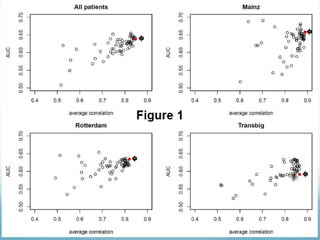
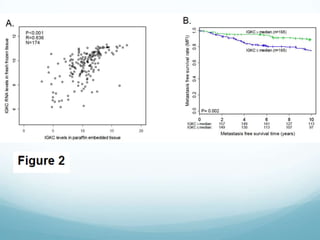
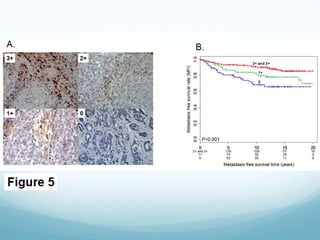
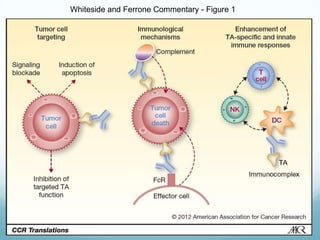
Hallmarks of IGKC
First Humoral Immunity Component studied
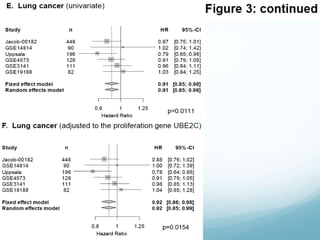
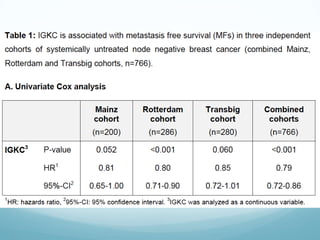
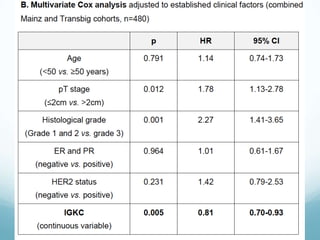
Predictive of Metastasis-Free Survival
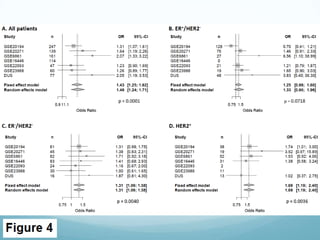
Response to chemotherapy (anthracycline)
Simplifies analysis from B cell metagene (60) to IGKC (1)
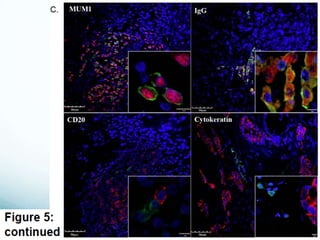
TA-specific Antibodies (?) – ADCC or Signalling
Plasma cell infiltrates vs. NK or T or Monocytes
Immune Score alternative to AJCC method
Tumor Clearance - B cell vs. T cell importance
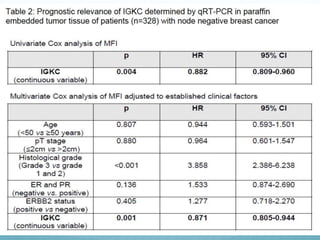
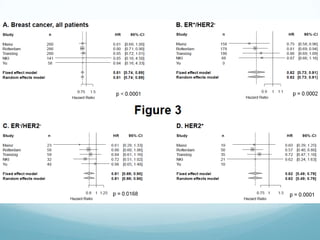
Conclusions
Positive prognosisand positive response to
neoadjuvant anthracycline chemotherapy treatment
Considered first immune gene signature relevant to
prognosis and treatment (others proliferation)
Implicates Humoral Immunity involved in tumor
microenvironment (not just cell-mediated)
27.
Discussion
This paperdistills down multiple metagene studies for
their results in finding a representative marker for
positive prognosis in the case of three forms of cancer.
What are some other prognostic indicators (negative or
positive), either discussed in the course of the paper or
from a quick search of the literature, that are commonly
used in cancer observation for either treatment or
survival?
28.
Question 2
TheWhiteside commentary that accompanied the
paper described the use of IGKC as a “silver bullet” of
sorts for genetic analyses where only one gene
representative of metastases free survival can be
studied representative of a whole 60-gene study of the
B-cell metagene. Is this a wise method to add to the
current practices of staging with an immune score
based on IGKC? Are there other factors to consider
that might call for other options in this case?
29.
Question 3
Withour recent lectures focusing on monoclonal
antibody treatments of cancer (humoral immunity
derived) and induced CTA expression as a method to
educate T cell-mediated immunity enhanced by
adoptive cell transfer, is there one system that seems
more effective in immunotherapy at this point, humoral
vs. cell-mediated, or is it too soon to know because
they are both in their infancy of study as treatment
options?
30.
Question 4
Concerningthe ideas of merging current staging
techniques for the characterization of tumors with the
immune markers discussed in the paper, Does this
paper make a significant case for the “emerging role of
the immune system as a clinically relevant hallmark of
cancer biology” from the standpoint of this biomarker?
31.
Question 5
TheSchmidt paper alludes to the hypothesis that
“chemotherapy does not only exert a direct cytotoxic
effect, but at the same time enhances the antitumor
immune response.” This thought is not new but further
substantiated by the correlation results of the study of
people with IGKC showing a positive response to
anthracycline neoadjuvant chemotherapy. Is it likely to
be useful in determining other treatment plans in
patients with adenocarcinoma or just in survival
outcomes?
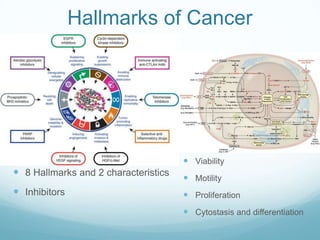
#4 Immune Hallmarks 1. Ability to thrive in a chronically inflamedmicroenvironment2. Ability to evade immune recognition3. Ability to suppress immune reactivity