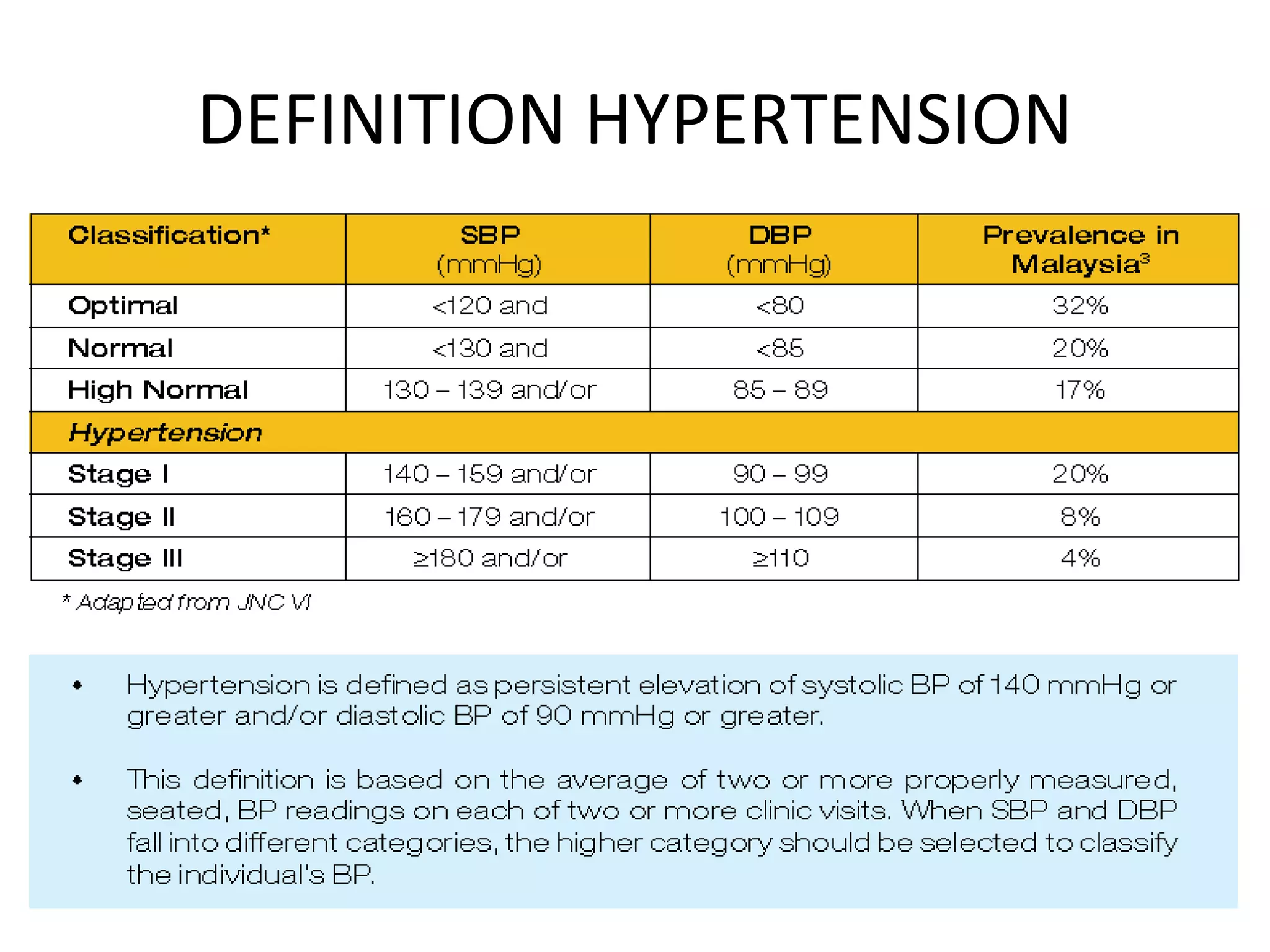
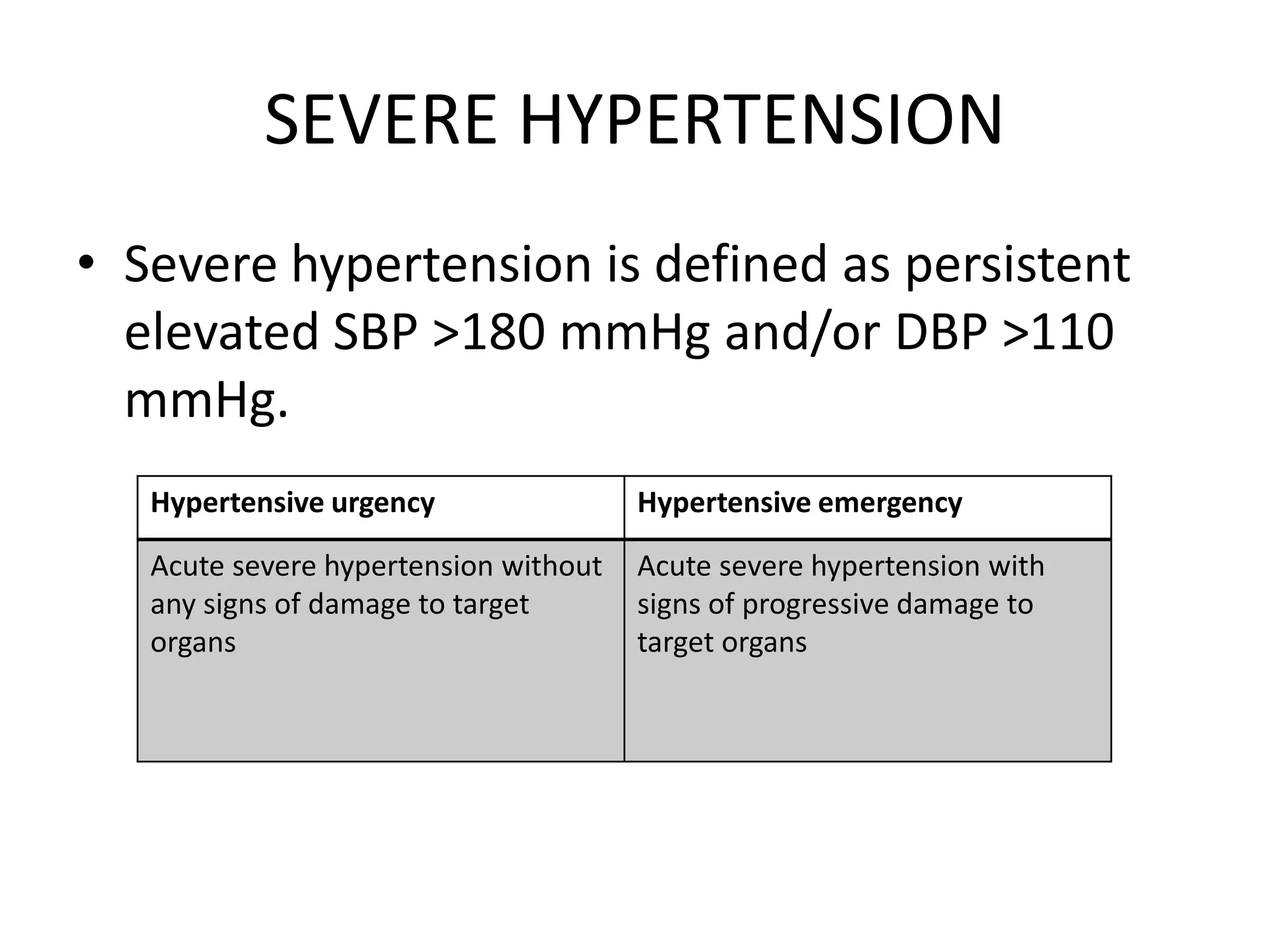
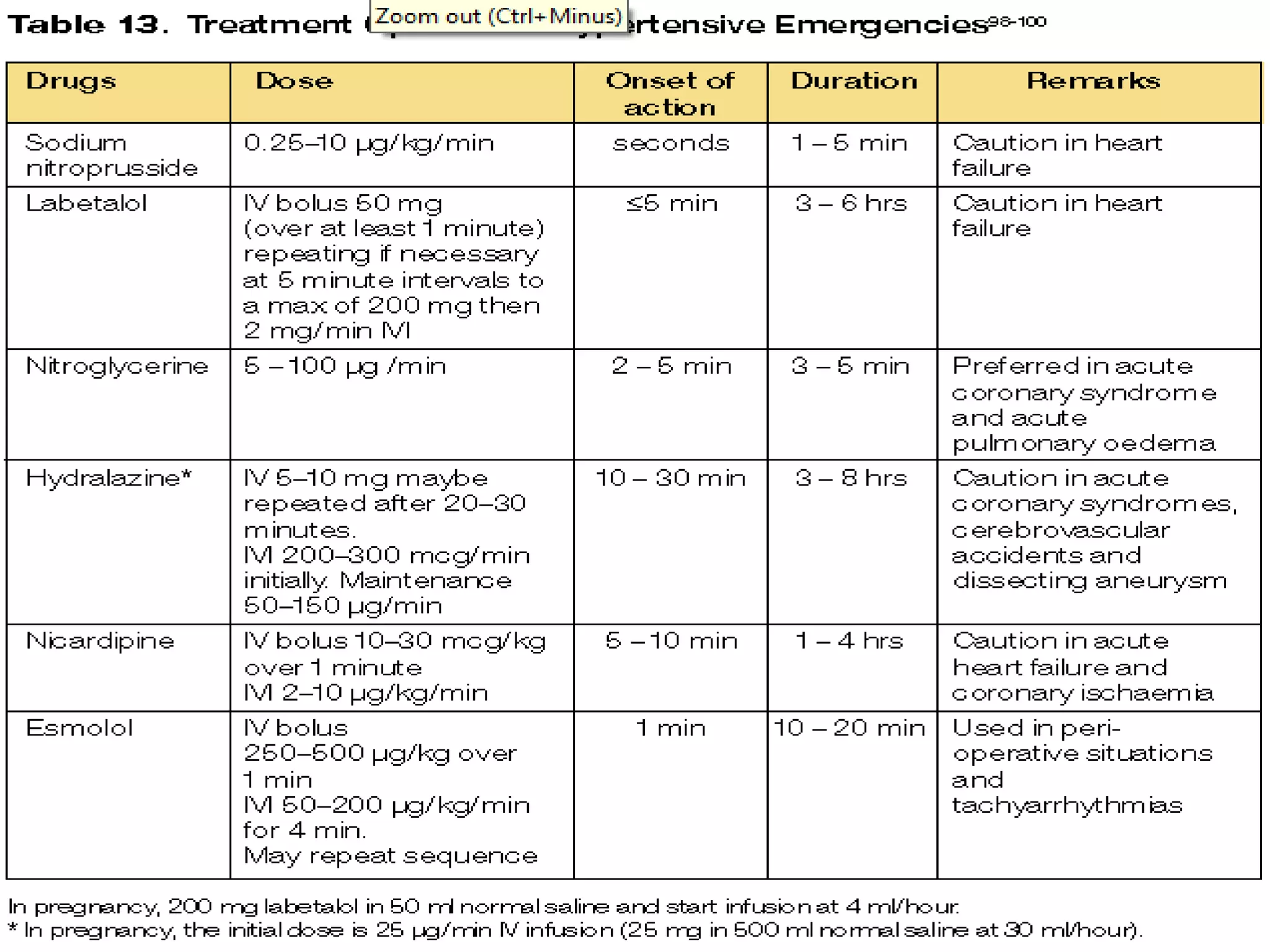
This document discusses hypertensive emergencies and urgencies. It defines severe hypertension and distinguishes between emergencies and urgencies. Hypertensive emergencies involve acute severe hypertension with signs of damage to target organs, while urgencies involve acute severe hypertension without organ damage. The document provides epidemiological data and discusses the etiology, pathophysiology, evaluation, and management of hypertensive crises. Management depends on the clinical presentation and involves rapidly reducing blood pressure in emergencies but more slowly in urgencies.