Download to read offline









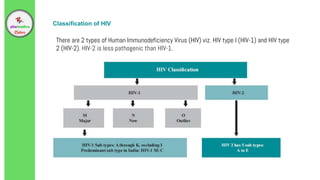



HIV is a virus that weakens the immune system by destroying CD4 cells. It can lead to AIDS if not treated. The document discusses HIV/AIDS including definitions, epidemiology in India, risk factors, transmission methods, the virus life cycle, stages of infection, signs and symptoms, diagnosis, and treatment approaches. It provides an overview of HIV from introduction through various treatment strategies and guidelines in India.






























































