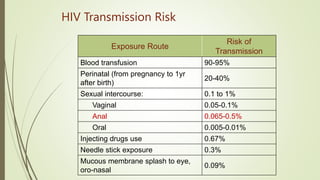
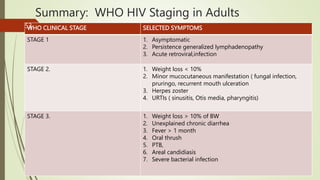
The document provides an educational overview of HIV/AIDS and STIs, aimed at enabling learners to define key terms, understand prevention and management strategies, and appreciate the impact of the disease on various populations. It outlines the historical background, prevalence statistics in Kenya, modes of transmission, and the effects of HIV on the immune system. The document also discusses the socio-cultural, biological, and behavioral factors contributing to the HIV epidemic and emphasizes the need for effective communication and community-based care.