

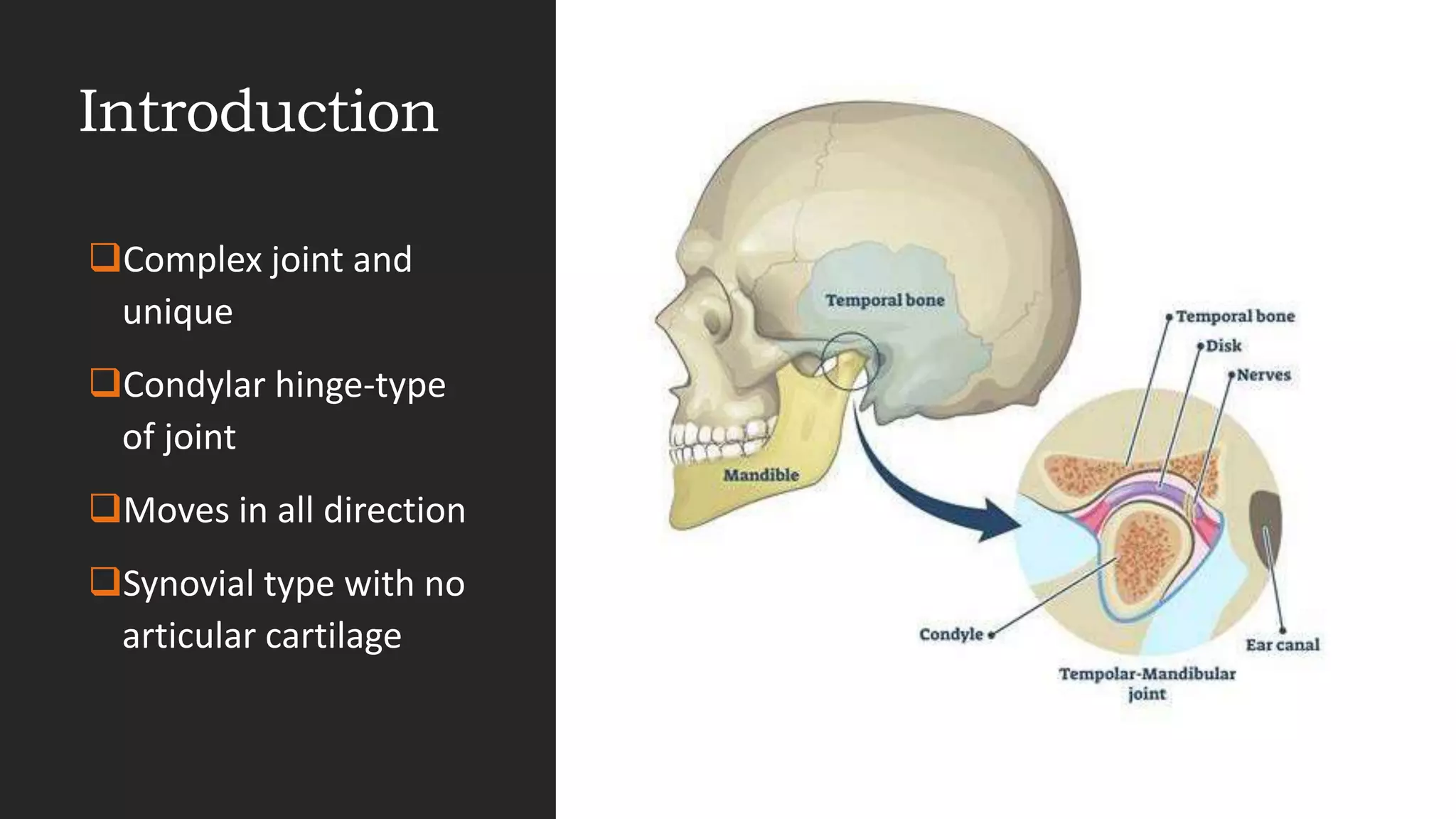
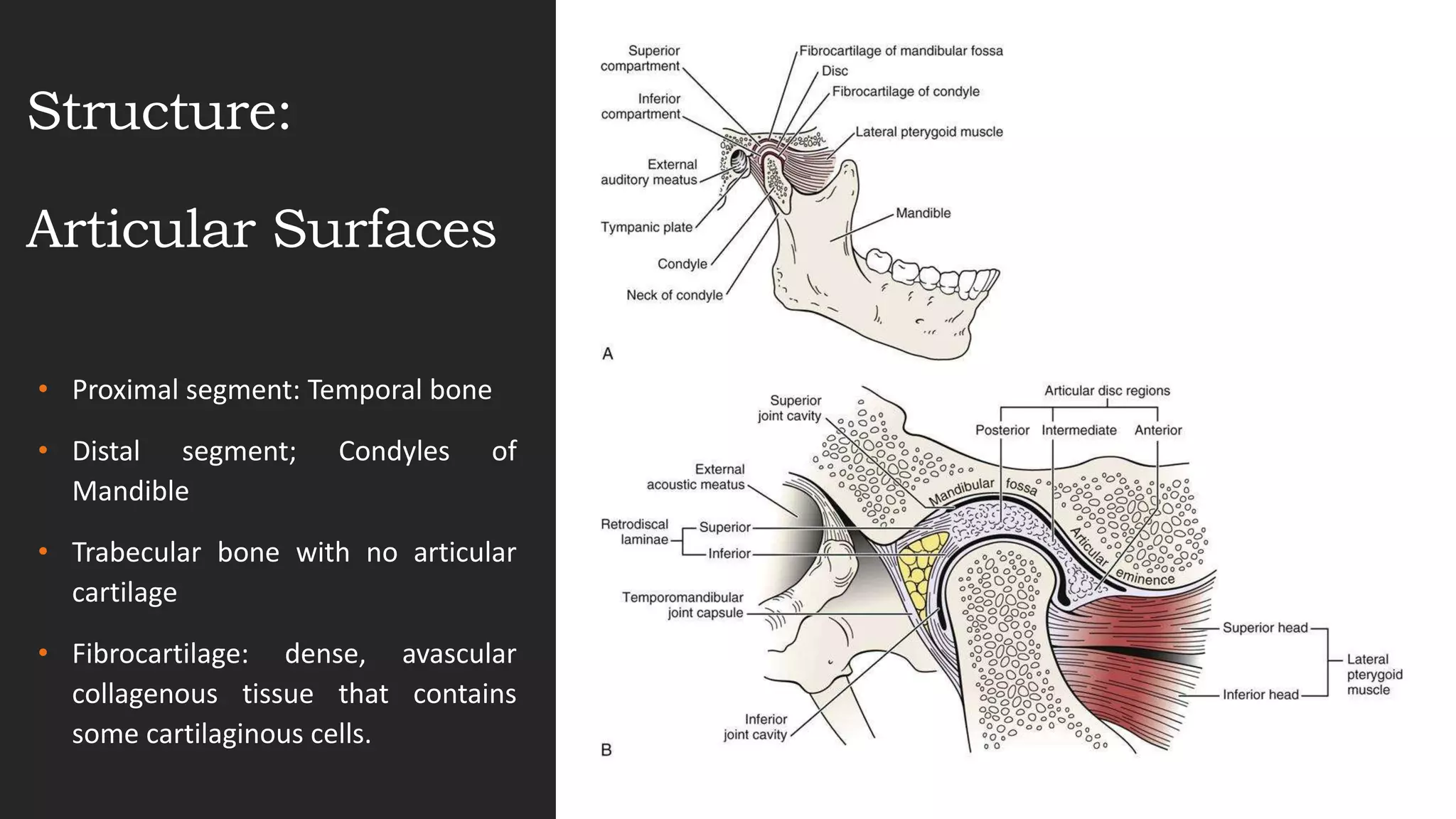

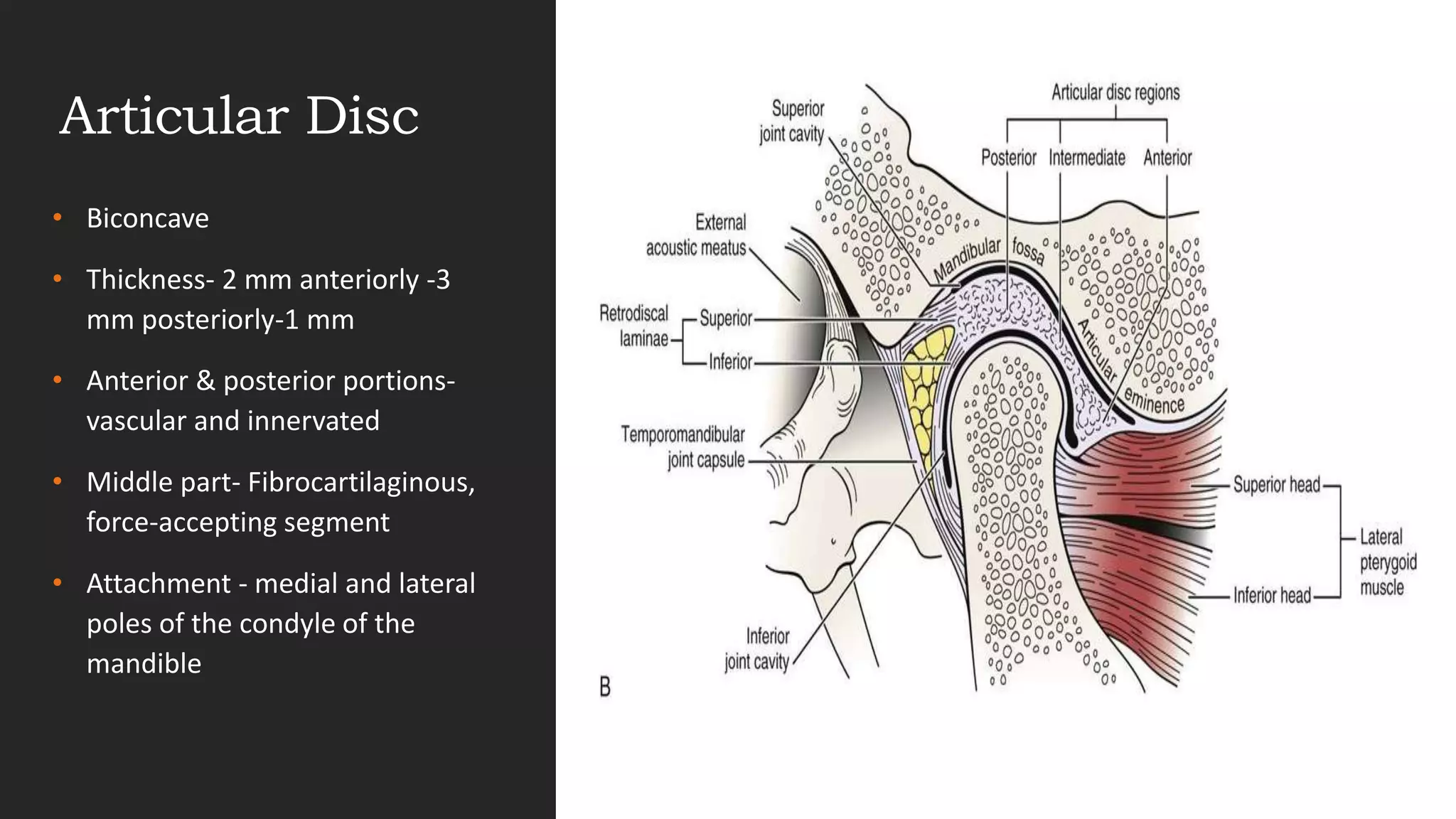


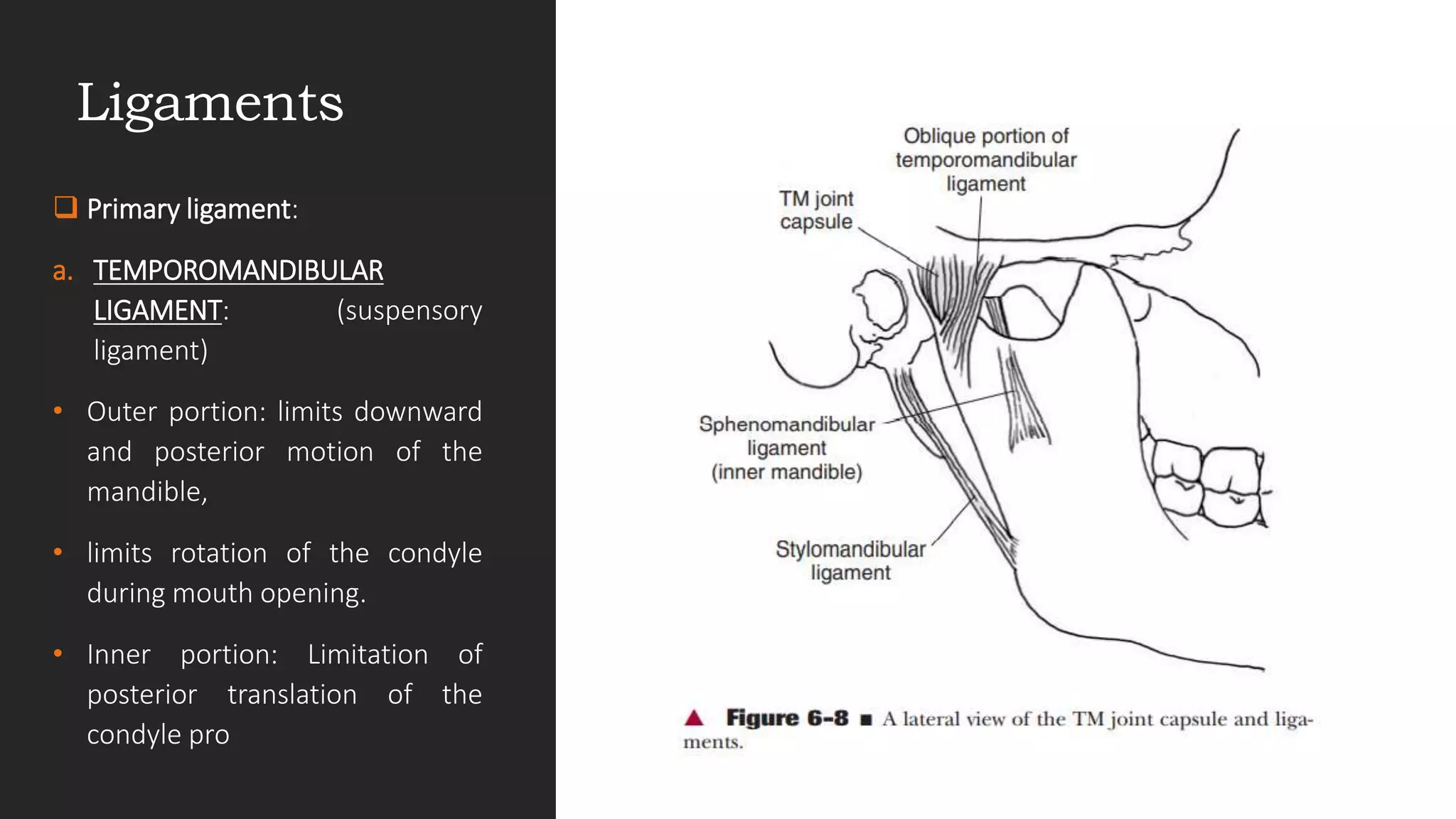



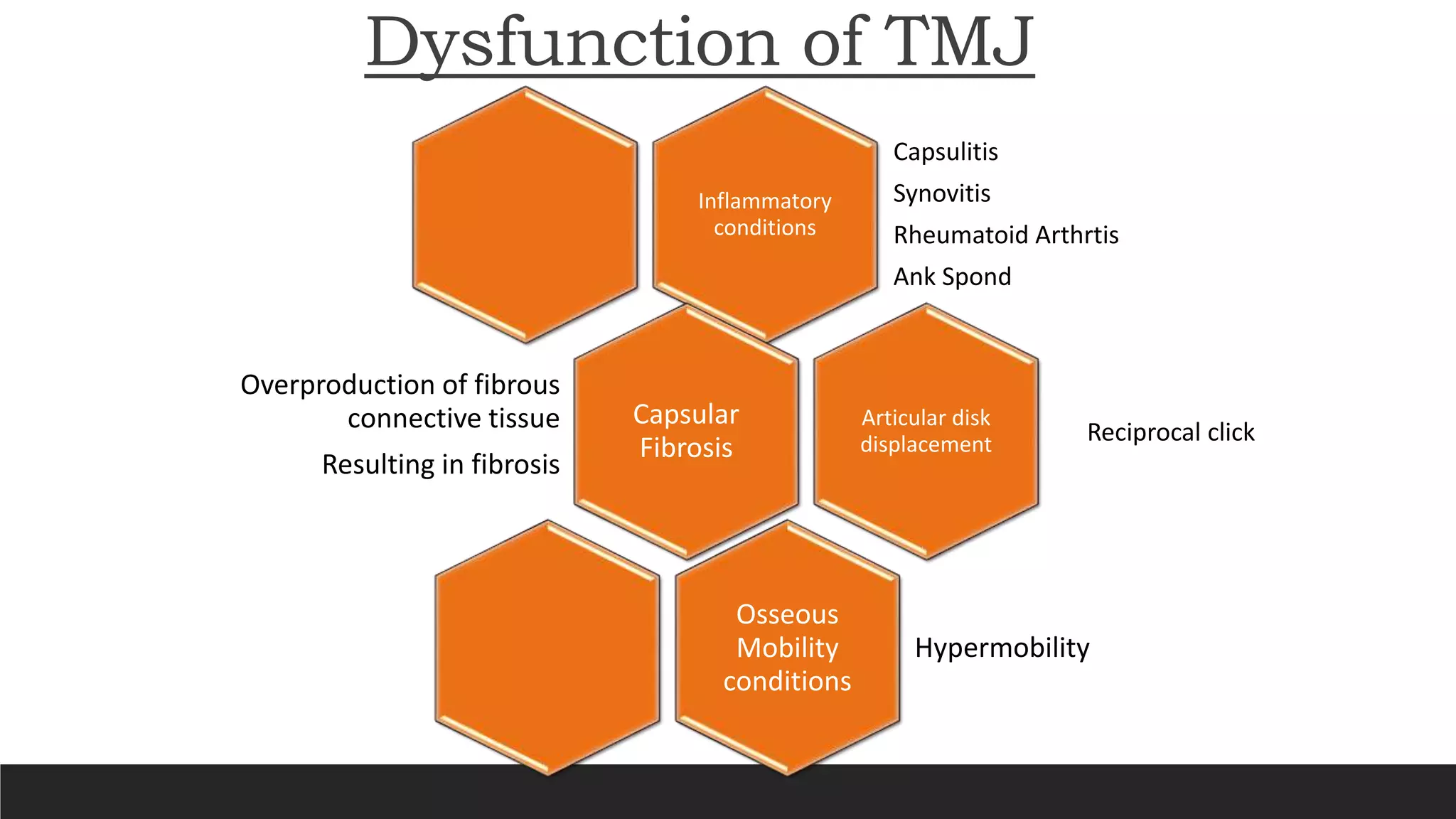



The document provides a comprehensive overview of the temporomandibular joint (TMJ), detailing its anatomy, structure, and functions. It describes the articular surfaces, ligaments, capsule, and the mechanics of jaw movements, as well as common dysfunctions such as capsulitis and articular disk displacement. The TMJ is essential for functions like talking, chewing, and swallowing and is subject to various inflammatory conditions and mobility issues.































![Temporomandibular joint [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/temporomandibularjointautosaved-230521065437-1cbd4148-thumbnail.jpg?width=640&height=640&fit=bounds)



















































