![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 2 of 23
EXECUTIVE SUMMARY
The Coordination Reform (2012-2015) of Norway was implemented on 1 January 2012 to 1) promote
a “more cohesive and coordinated approach to health and care services”, 2) apportion more health
and care services to the local municipalities, and 3) focus on “preventative measures and improving
public health” at local municipal level1
.
The policy reform was necessary because attempts to improve coordination between various sectors
of healthcare had been brewing since 1930s2
, as the “supply of health care [was] often fragmented,
with little coordination between providers and between levels of care”3
.
Improved coordination was projected to benefit patients by reducing waiting time to obtain
specialist treatment; introduction of the new concept of having one person as the main point-of-
contact in charge of organising health and care needs throughout the patient pathway; and disease
prevention by promoting healthy lifestyles at the community level.
To assess health inequalities arising from this intervention, an Equity-Focused Health Impact
Assessment (EFHIA) was carried out to consider “adverse and beneficial health effects”4
, as well as
“provide decision-makers with options”5
on how to address ensuing insights.
The objective of this EFHIA is to identify how the Coordination Reform may negatively or positively
impact upon the resident population of Norway, and assess the nature, timing, size and likelihood of
the impacts, to evaluate and outline recommendations to “alleviate the problems and challenges of
coordinating health and social care services”6
between Norway’s primary and secondary/tertiary
1
1. Norway TRCo. About the evaluation of the Coordination Reform. Oslo2012 [cited 2013 28
September]; Available from: http://www.forskningsradet.no/prognett-
evasam/The_evaluation/1253972204894.
2
2. Angell SI. Two variants of decentralised health care: Norway and Sweden in comparison. 2012 [cited
2013 25 September]; Available from: https://bora.uib.no/bitstream/handle/1956/6004/WP%2004-
20012%20Angell.pdf?sequence=1
3
3. Cristina Masseria RI, Sarah Thomson, Marin Gemmill and Elias Mossialos. Primary Care in Europe.
2009 [cited 2013 6 September]; Available from:
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&frm=1&source=web&cd=1&ved=0CC8QFjAA&url=http%3
A%2F%2Fec.europa.eu%2Fsocial%2FBlobServlet%3FdocId%3D4739%26langId%3Den&ei=hUWrUKXDNIfmrAeS
4oCYCw&usg=AFQjCNErLqS7id4v1lAyMUS6NFfayG8uhQ.
4
4. Prevention CfDCa. Health Impact Assessment. Atlanta2013 [cited 2013 5 October]; Available from:
http://www.cdc.gov/healthyplaces/hia.htm.
5
5. Organisation WH. The role of HIA in decision making. 2013 [cited 2013 19 October]; Available from:
http://www.who.int/hia/policy/decision/en/index.html.
6
6. Mawa BD. Coordination of Health and Social Care Services between Primary and Secondary health
and social care institutions in the Eastern Regional Health Enterprise (RHE) : The coordination challenges and](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-2-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 3 of 23
healthcare sectors; ensure responsibilities of disease prevention and health promotion are well-
managed by the local municipal administrations; and weigh the potential sequential differential
health impacts.
Equity would be defined as equal accessibility by Norwegian residents to the Norwegian healthcare
system, i.e.: populations across the social gradient are able to obtain the same high standard of care
and continuity in care, regardless of their mental or physical health status, geographical location or
age.
The Coordination Reform’s main thrust in “changing the municipalities’ role so that they can fulfil
the aims of prevention and early intervention while addressing the needs of patients with chronic
diseases”, aptly reinforces the 1978 Declaration of Alma-Ata to “provid[e] promotive, preventive,
curative and rehabilitative services accordingly”7
.
The population likely to be affected are residents and citizens living in Norway, with differential
health impacts most intensely felt in the following vulnerable groups: the elderly, mentally or
physically handicapped, patients with chronic or complex diseases, people who depend on carers,
and Culturally and Linguistically Diverse (CALD) populations.
The approach chosen for the EFHIA is desk-based, due to the relatively small number of health
impacts concerned, the mainly administrative nature of the reforms, and the time and resource
constraints involved. Qualitative research methods via grey literature reviews and existing
systematic reviews were employed. Professional stakeholders and community representatives from
vulnerable groups were included on the Steering Committee and consulted on relevant issues to
collate diverse perspectives.
problems in the mental health and social care sector for long term mental patients. 2007 [cited 2013 22
September]; Available from: https://www.duo.uio.no/handle/123456789/30334.
7
7. Office of the United Nations High Commissioner for Human Rights tWHO. The Right to Health: Fact
Sheet No. 31. Geneva2008 [cited 2013 7 September]; Available from:
http://www.ohchr.org/Documents/Publications/Factsheet31.pdf.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-3-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 4 of 23
Put forth are recommendations to enhance the potential positive health impacts, and mitigate
negative ones, i.e.: national inclusion of all GPs into the Norwegian Health Net8
for equal access to
specialist referrals across the secondary and tertiary sectors; national embrace of telemedicine9
to
allow both rural and urban populations with chronic diseases to benefit from e-health; subsidies for
dental care as dental health has a role in infections and diseases10
; provide guidelines on the
processes of organising care coordinators in the primary sector; establish a centralised database
body to collect data on health promotion activities that “reduce modifiable risk factors, often the
cause of costly chronic diseases”11
for evaluation and assessment purposes .
The limitations of this EFHIA were that there were a lack of similar HIAs for reference and reviews;
the findings are not replicable or reproducible as in a laboratory experiment; comparisons with other
quantitative assessments and “with standards are difficult since there are no common metrics”.
Recommendations arising from this HIA may be difficult to support “against quantitative ‘scientific’
data”, i.e.: economics, which brought the policy reform to the forefront.12
8
8. Ilkka Winblad JR, Sinikka Salo, Mary Wakeling, Anne Roberts, Eva Lindh Waterworth,, Ulla-Maija
Pesola FL, Bente Christensen, Minna Mäkiniemi and Anne MacFarlane. Utilization of the eHealth
Implementation Toolkit: Identification of pilot services in Finland, Scotland, Sweden and Norway. 2007 [cited
2013 20 October]; Available from:
http://www.ehealthservices.eu/instancedata/prime_product_julkaisu/npp/embeds/23411_e-
HIT_report_Final_ALL_PARTNERS.pdf.
9
9. Norway NCfTaUHoN. eHealth solutions across the Northern Periphery. 2013 [cited 2013 8
September]; Available from:
http://www.northernperiphery.eu/files/archive/Downloads/Project_Publications/11/Competitive%20Health%
20Services%20brochure.pdf.
10
10. Natale Rd. Sink your teeth into dental care reform. 2011 [cited 2013 5 September]; Available from:
http://www.abc.net.au/unleashed/3208234.html.
11
11. Goetzel RZ. Do Prevention Or Treatment Services Save Money? The Wrong Debate. 2012 [cited 2013
22 October]; Available from: http://content.healthaffairs.org/content/28/1/37.full.
12
12. Health USoP. Methodology: Models (taxonomy of HIA). Los Angeles2006 [cited 2013 27 September];
Available from: http://www.ph.ucla.edu/hs/health-impact/models.htm.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-4-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 5 of 23
SCREENING
The Coordination Reform intends to bring disease prevention and health promotional activities
closer to the people by assigning them to the local municipals, and enhance patient clinical care
pathways by improving the communication and coordination between primary health and long-term
care (under the local jurisdiction of 430 local municipalities), and hospitals and specialist services
(under state jurisdiction).
Norway’s 2-tiered healthcare system has led to a “highly fragmented [healthcare system which has
resulted in] in poor vertical and horizontal integration … focused on curing single diseases instead of
managing patient populations”13
. It is further aggravated by “different systems of funding,
administrative, political and professional cultures” [whereby] the specialist health care sector has
high competence, and … [is] … highly medical and diagnostic intensive, [whereas] municipality health
services are characterized by lower skills, [with up to] 29% of the [labour] force … [filled] by
personnel without appropriate formal health professional education, mostly in long-term care”14
.
Furthermore, the Coordination Reform seeks to address the fiscal problem of Norway’s ranking at
“among the highest [in terms of public health spending per capita] of all OECD nations [5388 USD
(adjusted for purchasing power parity), well above the OECD average of 3268 USD, or 9.4% of GDP in
2010]15
– [but without achieving] a correspondingly high level of health in return”16
.
Set against a backdrop of an aging population, longer queues for specialist healthcare treatment and
rises in chronic diseases, substance abuse problems and mental health disorders, the current
Norwegian healthcare system was deemed unsustainable and required strengthening of
coordination among the healthcare sectors to “ensur[e] the sustainability of the Norwegian welfare
system and the Norwegian National Insurance Scheme for future generations”17
.
13
13. Sophia Schlette ML, Kerstin Blum. Integrated primary care in Germany: the road ahead. International
Journal of Integrated Care. 2009;9(14).
14
14. Tor Inge Romøren DOT, Brynjar Landmark. Promoting coordination in Norwegian health care. Ibid.
2011;11(Special 10th Anniversary Edition).
15
15. OECD. OECD Health Data 2013: How Does Norway Compare. 2013 [cited 2013 11 October]; Available
from: http://www.oecd.org/norway/BriefingNoteNORWAY2012.pdf.
16
16. Hanssen BH. The Coordination Reform: Proper treatment – at the right place and right time.
Norwegian Ministry of Health and Care Services; 2009 [cited 2013 11 September]; Available from:
http://www.regjeringen.no/upload/HOD/Dokumenter%20INFO/Samhandling%20engelsk_PDFS.pdf.
17
16. Ibid.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-5-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 6 of 23
This policy reform focuses on the health determinants of access and use of health care services, and
health promotion to influence modifiable disease-risk lifestyle behaviours.18
Assumptions of the reform include: suppositions that all Norwegian residents know of the
Coordination Reform’s existence and seek appropriate medical treatment and care; equal
accessibility to healthcare despite wide disparities in SES across the country; and ability by rural
populations to have financial or transportation means to access healthcare services.
Health impacts include faster medical treatment from shorter waiting time due to improved
coordination between primary and secondary / tertiary healthcare sectors; and a potential reduction
in NCDs from healthier lifestyles arising from health promotion at local community level.
Relevant information pertaining to the nature and extent of the impacts of health for the
Coordination Reform has been gathered from several sources, to wit:
– grey literature derived from government sources, e.g.:
- “The Coordination Reform”19
– existing systematic reviews, e.g.:
- “ Nordic Heath Care Systems: Recent Reforms and Current Policy Changes”20
- “Is the increasing policy use of Impact Assessment in Europe likely to undermine
efforts to achieve healthy public policy?”21
- “Cooperation and Coordination in Health Care”22
18
17. Organisation WH. The determinants of health. 2013 [cited 2013 13 September]; Available from:
http://www.who.int/hia/evidence/doh/en/
19
16. Hanssen BH. The Coordination Reform: Proper treatment – at the right place and right time.
Norwegian Ministry of Health and Care Services; 2009 [cited 2013 11 September]; Available from:
http://www.regjeringen.no/upload/HOD/Dokumenter%20INFO/Samhandling%20engelsk_PDFS.pdf.
20
18. Policies EooHSa. Nordic Heath Care Systems: Recent Reforms and Current Policy Changes. 2009 [cited
2013 13 September]; Available from:
http://www.euro.who.int/__data/assets/pdf_file/0011/98417/E93429.pdf.
21
19. Katherine E Smith GF, Jeff Collin, Heide Weishaar, Anna B Gilmore. Is the increasing policy use of
Impact Assessment in Europe likely to undermine efforts to achieve healthy public policy? J Epidemiol
Community Health. 2010;64(6):478-87.
22
20. Dag Olaf Torjesen ABH. Cooperation and Coordination in Health Care. 2011 [cited 2013 9
September]; Available from: https://conference.cbs.dk/index.php/nohr/health/paper/viewFile/999/449.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-6-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 7 of 23
The Coordination Reform listed the "elderly, and increasing numbers of people with chronic and
complex illnesses [such as] COPD, diabetes, dementia, cancer and mental disorders [which] are all
increasing sharply [and represent] large patient groups with a growing need for coordination"23
as
vulnerable groups and beneficiaries of the policy.
Additional vulnerable groups identified over the course of this HIA include: “people with special
needs and various levels of dependency such as children with special needs and the physically or
mentally handicapped”24
, single-member households with no carers, rural populations, and
Culturally and Linguistically Diverse (CALD) groups.25
This “inequality of access is particularly disturbing since medical conditions and treatments such as
organ transplantations … defined as having a high medical and political priority in the Norwegian
National Health Service” would be even more inaccessible to these vulnerable groups.26
Thus, the
challenge is to achieve geographical (and health) equity while “exploiting both medical and
economic scale efficiencies”27
.
Health impacts are expected to benefit vulnerable groups who require specialist or frequent medical
attention the most.
The Coordination Reform warrants an EFHIA as there are always “conflicts involved in balancing
economic, social and [health] considerations”28
.
23
21. Services NMoHaC. The Coordination Reform: Proper treatment – at the right place and right time.
2009 [cited 2013 8 September]; Available from:
http://www.regjeringen.no/upload/HOD/Samhandling%20engelsk_PDFS.pdf.
24
13. Sophia Schlette ML, Kerstin Blum. Integrated primary care in Germany: the road ahead. International
Journal of Integrated Care. 2009;9(14).
25
22. Prevention and Population Branch W, Integrated Care & Ageing Division of the Victorian State
Government, Department of Health, Australia. The determinants of health. 2011 [cited 2013 17 September];
Available from: http://www.health.vic.gov.au/healthpromotion/what_is/determinants.htm.
26
23. Knut Rasmussen DB. Quality or equality? The Norwegian experience with medical monopolies. 2007
[cited 2013 15 September]; Available from: http://www.biomedcentral.com/1472-6963/7/20/table/T3.
27
18. Policies EooHSa. Nordic Heath Care Systems: Recent Reforms and Current Policy Changes. 2009 [cited
2013 13 September]; Available from:
http://www.euro.who.int/__data/assets/pdf_file/0011/98417/E93429.pdf.
28
19. Katherine E Smith GF, Jeff Collin, Heide Weishaar, Anna B Gilmore. Is the increasing policy use of
Impact Assessment in Europe likely to undermine efforts to achieve healthy public policy? J Epidemiol
Community Health. 2010;64(6):478-87.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-7-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 8 of 23
SCOPING
The Steering Committee comprised of the relevant stakeholders from:
• The Norwegian Board of Health Supervision29
1. The Director as Chairperson, chosen for vast experience in policy analysis and high-level
cooperation amongst various government agencies (Norwegian Directorate of Health, The
Norwegian Institute of Public Health, and the Norwegian Registration Authority for Health
Personnel) to handle potential conflicts between other members of the Steering Committee
2. A senior social worker, to hear his / her opinions and experiences on working with people
with acute or chronic health problems which require complex or long-term supervision or
coordination
• The Ministry of Health
2. Bjarne Håkon Hanssen, Minister of Health and Social Affairs30
, who presented the
Coordination Reform to the Norwegian Parliament (Storting) in 2009
• The Norwegian Institute of Public Health31
3. An epidemiologist (public health professional)
• Oslo University Hospital32
4. An ophthalmologic transplant surgeon (specialist)
• A rural municipality in Artic Norway
5. a resident from Northern Norway, e.g.: Tromsø, the “capital of the Artic”33
29
24. Helsetilsyn S. Norwegian Board of Health Supervision. 2010 [cited 2013 20 September]; Available
from: https://www.helsetilsynet.no/no/Norwegian-Board-of-Health-Supervision/Organization/#countyorg.
30
25. Services MoHaC. The Coordination Reform. Oslo2008 [cited 2013 3 September]; Available from:
http://www.regjeringen.no/en/archive/Stoltenbergs-2nd-Government/ministry-of-health-and-care-
services/tema-og-redaksjonelt-innhold/kampanjesider/2008/the-coordination-reform.html?id=524777.
31
26. Health TNIoP. The Norwegian Institute of Public Health. Oslo2013 [cited 2013 2 September];
Available from: http://www.fhi.no/eway/?pid=238.
32
27. Universitetssykehus O. Department of Ophthalmology Oslo2013 [cited 2013 2 September]; Available
from: http://www.oslo-universitetssykehus.no/OMOSS/ENGLISH/ORGANISATIONAL-UNITS/Sider/department-
of-ophthalmology.aspx.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-8-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 9 of 23
• The aging population
6. a senior citizen aged >65 years old, perhaps recruited from the eldresenter (senior citizens'
community centre or seniors centre)34
• The mental disorders / substance abuse and addiction community
7. current or previous patient under medical treatment for mental disorders or substance
abuse, for his / her perspectives on the difficulties encountered in obtaining appropriate and
timely medical and health care
These 8 people were specifically selected as the Steering Committee needed to be of a size that was
manageable, yet large enough to include a diverse range of perspectives and expertise.
Core values are that there must be neither conflict of interest nor financial benefit from advocacy
from any angle. Health equity is defined as equal access to health care services regardless of social
determinants. (Proper treatment – at the right place and right time35
)
Evidence presented would be discussed by the Steering Committee in a civilised and logical manner,
and treated as a fact-finding mission. Conflicting evidence would be resolved by holding qualitative
discussions with community representatives. Where impact in literature differs from perceived
impact, community concerns would be addressed by publicising research findings, to facilitate the
transparency of the EFHIA.
‘Off the shelf’ resources such as grey literature reviews and systematic reviews for “synthesising and
appraising information”36
would form the bulk of data analysis.
A ‘desk-based’ approach is taken for this EFHIA, because only 2 health impacts, i.e.: access and use
of health care services, and health promotion, have been identified for reform. Differential and
unintended impacts identified by the Steering Committee would be subjected to recommendations,
with respect to the findings and discussions.
Typologies of evidence used would be Demographic Analysis to identify the Differential Impacts of
the Coordination Reform; The Effect and Use of the Coordination Reform is going to be gathered
from every member of the Steering Committee, in particular the proponents and decision-makers of
33
28. Norway I. Tromsø. 2013 [cited 2013 22 September]; Available from:
http://www.visitnorway.com/en/Where-to-go/North/Tromso/.
34
29. Kommune O. Senior Citizen's Community. Oslo2011 [cited 2013 22 September]; Available from:
http://www.oslo.kommune.no/english/health_/senior_citizens/.
35
30. Services MoHaC. Ministry of Health and Care Services. Oslo2012 [cited 2013 5 September]; Available
from: http://www.regjeringen.no/en/dep/hod.html?id=421.
36
31. Harris P, Harris-Roxas, B., Harris, E., & Kemp, L. Health Impact Assesessment: A practical guide.
Sydney: Centre for Health Equity Training, Research and Evaluation, University of New South Wales 2007.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-9-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 10 of 23
the healthcare policy reform (i.e.: Director of the Norwegian Board of Health Supervision, the
Minister of Health and Social Affairs of Norway).
In addition, as the overhaul is meant to reform the “lack of contact between hospitals and local
authorities” in the Norwegian healthcare system37
to benefit patients, opinions on the Salience and
Satisfaction by the 3 vulnerable groups representatives and social worker in the Steering Committee
would be given slightly higher weightage, as they represent affected populations.
37
25. Services MoHaC. The Coordination Reform. Oslo2008 [cited 2013 3 September]; Available from:
http://www.regjeringen.no/en/archive/Stoltenbergs-2nd-Government/ministry-of-health-and-care-
services/tema-og-redaksjonelt-innhold/kampanjesider/2008/the-coordination-reform.html?id=524777.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-10-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 11 of 23
POPULATION PROFILE
The population of Norway stands at approximately 5 million, with low population density of 16
inhabitants / km2
. The 5 main counties of Akershus, Hordaland, Oslo, Rogaland and Sør-Trøndelag
contain nearly ½ of the country’s population, while the other 14 counties contain the other ½.38
Life expectancy is 83 years for females, and 79 years for males, with an immigrant population at
10.2% of the total population.39
The elderly population is a burgeoning healthcare burden, as age is an important risk factor for
dementia and other NCDs. CVDs remain the most common cause of death for elderly aged >65years
old, amounting to 35% of all deaths annually.40
Less than 20% of the total female / male population smoke41
, with those who smoke predominantly
“amongst populations with lower education and income”42
. Approximately 1/5 of females and 1/3 of
males are overweight / obese.43
10% of the working population claims disability pension, indicating a sizable number incapacitated
by physical and/or mental illnesses. “Skeletal and muscular diseases combined with pain, and mental
illnesses” contribute enormously “to these high figures, resulting in a significant number of lost
38
32. Norway S. Minifacts about Norway 2013: Demographics, health and crime. 2013 [cited 2013 7
September]; Available from:
http://www.ssb.no/english/subjects/00/minifakta_en/en/main_03.html#tab0301.
39
32. Ibid.
40
33. Health NIoP. Health among the elderly (65 years and over) in Norway - fact sheet. 2013 [cited 2013
11 September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7630:1:0:0:::0:0&Main
Content_6894=6671:0:25,7646:1:0:0:::0:0&List_6673=6674:0:25,7658:1:0:0:::0:0.
41
32. Norway S. Minifacts about Norway 2013: Demographics, health and crime. 2013 [cited 2013 7
September]; Available from:
http://www.ssb.no/english/subjects/00/minifakta_en/en/main_03.html#tab0301.
42
34. Health NIoP. Smoking and smokeless tobacco in Norway - fact sheet. 2013 [cited 2013 11
September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7629:1:0:0:::0:0&Main
Content_6894=6671:0:25,7640:1:0:0:::0:0&List_6673=6674:0:25,7751:1:0:0:::0:0.
43
32. Norway S. Minifacts about Norway 2013: Demographics, health and crime. 2013 [cited 2013 7
September]; Available from:
http://www.ssb.no/english/subjects/00/minifakta_en/en/main_03.html#tab0301.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-11-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 12 of 23
working years”. Moreover, “at any given time, 30% of the adult population suffer from chronic pain,
where prevalence increases with age, and women are more exposed than men”44
.
93.3% of deaths are caused by NCDs, whereby malignant tumours, heart and circulatory diseases,
and respiratory diseases account for the main causes. Violent deaths from accidents, suicides and
homicides made up the remaining 6.1%.45
Anxiety, depression, drug abuse and addiction are the most common mental illnesses in Norway,
with 5% of the population suffering from alcoholism. “Good social networks, both in the local
community and at work, are important factors for maintaining good health, [as] limited social
support reduces the ability to deal with stress and has a direct negative impact on health and quality
of life. People lacking close familiar relations have higher mortality, especially … CVDs, [thus] support
from family, friends and colleagues is important to both mental and somatic health”46
.
SES plays a huge role in determining health: “Improvements [in health and life expectancy] have
been greater for groups with higher education and higher income than for those with lower
education and lower income.“ Hence, it cannot be assumed that universal healthcare equates to
equally good health for all.47
44
35. Health NIoP. Chronic pain prevalence in Norway – fact sheet. 2013 [cited 2013 9 September];
Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7583:1:0:0:::0:0&Main
Content_6894=6671:0:25,7590:1:0:0:::0:0&List_6673=6674:0:25,7602:1:0:0:::0:0.
45
32. Norway S. Minifacts about Norway 2013: Demographics, health and crime. 2013 [cited 2013 7
September]; Available from:
http://www.ssb.no/english/subjects/00/minifakta_en/en/main_03.html#tab0301.
46
36. Health NIoP. Psychological problems and disorders in Norway - fact sheet. 2013 [cited 2013 9
September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7583:1:0:0:::0:0&Main
Content_6894=6671:0:25,7587:1:0:0:::0:0&List_6673=6674:0:25,7593:1:0:0:::0:0.
47
37. Health NIoP. Education level and health in Norway - fact sheet. Oslo2013 [cited 2013 9 September];
Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7630:1:0:0:::0:0&Main
Content_6894=6671:0:25,7643:1:0:0:::0:0&List_6673=6674:0:25,7649:1:0:0:::0:0.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-12-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 13 of 23
EVIDENCE APPRAISAL
Evidence appraisal includes systematic and grey literature reviews (listed in the Screening section
above), as well as analyses of similar healthcare reforms in 5 other countries, to wit, Sweden48
,
Denmark49
, Canada50
, Australia51
, and the UK52
.
IMPACT ASSESSMENT
If systematic review evidence is more highly valued than other evidence, then the EFHIA tells us that:
participation of all GPs need to be more inclusive so standard of care is not GP-dependent53
;
existing ad-hoc telemedicine services should be nationally, rather than sporadically,
available to all residents to be equitable 54 55
;
48
14. Tor Inge Romøren DOT, Brynjar Landmark. Promoting coordination in Norwegian health care.
International Journal of Integrated Care. 2011;11(Special 10th Anniversary Edition).
49
14. Ibid.
50
38. Health-e-Solutions. Overview of Canada’s Health Care System. 2010 [cited 2013 5 September];
Available from: http://www.healthesolutions.ca/wp-content/uploads/2011/01/MB-Overview-of-Canadas-
Health-Care-systems.pdf.
51
39. Labor N. Right care Right place Right time. Sydney2011 [cited 2013 4 September]; Available from:
http://www.parliament.nsw.gov.au/prod/web/common.nsf/cbe381f08171c2e8ca256fca007d6044/365ca6edd
5c453a5ca25788f00048421/$FILE/ATTG75Q2.pdf/Appendix%2012%20-
%20Right%20Care,%20Right%20Place,%20RightTime.pdf.
52
40. Improvement NIfIa. Quality and Service Improvement Tools: Reliable Design. 2012 [cited 2013 13
September]; Available from:
http://www.institute.nhs.uk/quality_and_service_improvement_tools/quality_and_service_improvement_too
ls/reliable_design.html.
53
8. Ilkka Winblad JR, Sinikka Salo, Mary Wakeling, Anne Roberts, Eva Lindh Waterworth,, Ulla-Maija
Pesola FL, Bente Christensen, Minna Mäkiniemi and Anne MacFarlane. Utilization of the eHealth
Implementation Toolkit: Identification of pilot services in Finland, Scotland, Sweden and Norway. 2007 [cited
2013 20 October]; Available from:
http://www.ehealthservices.eu/instancedata/prime_product_julkaisu/npp/embeds/23411_e-
HIT_report_Final_ALL_PARTNERS.pdf.
54
41. Telemedicine NCfICa. The Norwegian Centre for Telemedicine. 2013 [cited 2013 20 October];
Available from: http://telemed.custompublish.com/about-nst.5108462-258955.html.
55
42. Telemedicine NCf. Innovation in e-Health and Telemedicine. 2013 [cited 2013 12 October]; Available
from: http://www.ehealthservices.eu/project_partners/nst.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-13-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 14 of 23
differential health impacts would not be equitably levelled by bureaucratic directives from
the Coordination Reform without first implementing nationally integrated ICT platforms
(e.g.: IHiS, HiMSS)56
;
advisory guidelines on implementing supportive working environments for HCWs assigned
to be the “one person as a contact point for all the services”57
to prevent mental health
impacts of HCW58
stress or burnout.
If grey literature review evidence is more highly valued than other evidence, then the EFHIA tell us
that:
people with special needs and various levels of dependency such as children with special
needs and the physically or mentally handicapped”59
, single-member households with no
carers, rural populations, and Culturally and Linguistically Diverse (CALD) groups have been
erroneously omitted as vulnerable groups;
assistance from Norwegian Institute of Public Health60
which has vast experience in health
promotion, such as advocating “long education, good income and [being] in a relationship”
for good health and providing physiotherapy at primary care level as a disease prevention
measure61
, should be extended to the 430 municipals on how to carry out health promotion
activities to reach as many people as possible which would otherwise be trial-and-error
attempts.
56
43. Systems HIaM. About HIMSS. Chicago2013 [cited 2013 5 October]; Available from:
http://www.himss.org/ASP/aboutHimssHome.asp.
57
21. Services NMoHaC. The Coordination Reform: Proper treatment – at the right place and right time.
2009 [cited 2013 8 September]; Available from:
http://www.regjeringen.no/upload/HOD/Samhandling%20engelsk_PDFS.pdf.
58
44. Canada TCBo. Enhancing Interdisciplinary Collaboration in Primary Healthcare in Canada. Ottawa2005
[cited 2013 28 October]; Available from: http://www.eicp.ca/en/resources/pdfs/enhancing-interdisciplinary-
collaboration-in-primary-health-care-in-canada.pdf.
59
13. Sophia Schlette ML, Kerstin Blum. Integrated primary care in Germany: the road ahead. International
Journal of Integrated Care. 2009;9(14).
60
37. Health NIoP. Education level and health in Norway - fact sheet. Oslo2013 [cited 2013 9 September];
Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7630:1:0:0:::0:0&Main
Content_6894=6671:0:25,7643:1:0:0:::0:0&List_6673=6674:0:25,7649:1:0:0:::0:0.
61
45. Physiotherapy TCSo. Public Health. London2012 [cited 2013 19 October]; Available from:
http://www.csp.org.uk/topics/public-health.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-14-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 19 of 23
RECOMMENDATIONS
Herein contains recommendations to even out potential differential health impacts under the
Coordination Reform (2012), for both patient pathway coordination and health promotion.
1. Include all GPs in the Norwegian Health Net (EMR), thus any patient who sees their registered
GP can be assured of fair and equal patient care coordination for referrals to specialists or
hospitals.
With most GPs already included in the Norwegian Health Net62
, a directive from the
Ministry of Health and Care Services and municipal funding channelled from the
Coordination Reform would rapidly enable the remaining GPs to be connected to the
Norwegian Health Net.
2. Roll out telemedicine nationwide to reach all regions of Norway, instead of being a project-
based, piecemeal option, relying on municipal / doctor interest for the take-up rate63
.
Telemedicine allows patients with chronic conditions to keep doctors updated in real-
time about their conditions, and only travel to the consult the doctor when necessary
This is to homogenise the access of health and care services in Norway across the
country, to make access to healthcare equal and fair for rural populations and
vulnerable groups such as the elderly and physically or mentally handicapped, who may
have difficulty accessing timely medical attention, due to age, medical condition, harsh
climate or remoteness.
The Norwegian Centre for Telemedicine is best positioned to advise on and implement
telemedicine across Norway
62
8. Ilkka Winblad JR, Sinikka Salo, Mary Wakeling, Anne Roberts, Eva Lindh Waterworth,, Ulla-Maija
Pesola FL, Bente Christensen, Minna Mäkiniemi and Anne MacFarlane. Utilization of the eHealth
Implementation Toolkit: Identification of pilot services in Finland, Scotland, Sweden and Norway. 2007 [cited
2013 20 October]; Available from:
http://www.ehealthservices.eu/instancedata/prime_product_julkaisu/npp/embeds/23411_e-
HIT_report_Final_ALL_PARTNERS.pdf.
63
8. Ibid.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-19-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 20 of 23
3. Subsidise expensive privatised dental treatment for adults as a disease prevention measure
To prevent many mental and physical health problems linked to oral infections64
Dental subsidies may be derived from funding channelled to municipalities from the
Coordination Reform for disease prevention at local community levels
The Ministry of Health and Care Services is best placed to negotiate with the Norwegian
Dental Association on agreeable subsidised co-payments schemes
4. Provide guidelines on which personnel in the primary care sector may best take on the new role
of patient pathway coordination, and how it should be done, to minimise teething problems in
the process of setting up care coordination65
To prevent HCW burnout and stress, by identifying who would best fill the role of care
coordinator; electronically manage patient care pathway to allow care coordinators to
assist one another and set automated digital alarms to enhance schedule adherence
The Ministry of Health and Care Services is best positioned to set guidelines
5. Establish one centralised body to keep track of the disease prevention and health promotion
activities of the 430 local municipalities
To enable cost-effective ways of reaching out to the public, through lateral transfer of
ideas from municipalities that have achieved success in reducing disease-risk behaviours
(such as alcohol addiction) and seen a reduction in NCDs caused by lifestyle changes
(regular physical activity, decreased obesity-related diseases, for example)66
To oversee and collate information for assessment and evaluation purposes
The Norwegian Institute of Public Health is best positioned to set up a central database
64
10. Natale Rd. Sink your teeth into dental care reform. 2011 [cited 2013 5 September]; Available from:
http://www.abc.net.au/unleashed/3208234.html.
65
21. Services NMoHaC. The Coordination Reform: Proper treatment – at the right place and right time.
2009 [cited 2013 8 September]; Available from:
http://www.regjeringen.no/upload/HOD/Samhandling%20engelsk_PDFS.pdf.
66
11. Goetzel RZ. Do Prevention Or Treatment Services Save Money? The Wrong Debate. 2012 [cited 2013
22 October]; Available from: http://content.healthaffairs.org/content/28/1/37.full.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-20-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 21 of 23
Bibliography
1. Norway TRCo. About the evaluation of the Coordination Reform. Oslo2012 [cited 2013 28
September]; Available from: http://www.forskningsradet.no/prognett-
evasam/The_evaluation/1253972204894.
2. Angell SI. Two variants of decentralised health care: Norway and Sweden in comparison.
2012 [cited 2013 25 September]; Available from:
https://bora.uib.no/bitstream/handle/1956/6004/WP%2004-20012%20Angell.pdf?sequence=1
3. Cristina Masseria RI, Sarah Thomson, Marin Gemmill and Elias Mossialos. Primary Care in
Europe. 2009 [cited 2013 6 September]; Available from:
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&frm=1&source=web&cd=1&ved=0CC8QFjAA&u
rl=http%3A%2F%2Fec.europa.eu%2Fsocial%2FBlobServlet%3FdocId%3D4739%26langId%3Den&ei=h
UWrUKXDNIfmrAeS4oCYCw&usg=AFQjCNErLqS7id4v1lAyMUS6NFfayG8uhQ.
4. Prevention CfDCa. Health Impact Assessment. Atlanta2013 [cited 2013 5 October]; Available
from: http://www.cdc.gov/healthyplaces/hia.htm.
5. Organisation WH. The role of HIA in decision making. 2013 [cited 2013 19 October];
Available from: http://www.who.int/hia/policy/decision/en/index.html.
6. Mawa BD. Coordination of Health and Social Care Services between Primary and Secondary
health and social care institutions in the Eastern Regional Health Enterprise (RHE) : The coordination
challenges and problems in the mental health and social care sector for long term mental patients.
2007 [cited 2013 22 September]; Available from:
https://www.duo.uio.no/handle/123456789/30334.
7. Office of the United Nations High Commissioner for Human Rights tWHO. The Right to
Health: Fact Sheet No. 31. Geneva2008 [cited 2013 7 September]; Available from:
http://www.ohchr.org/Documents/Publications/Factsheet31.pdf.
8. Ilkka Winblad JR, Sinikka Salo, Mary Wakeling, Anne Roberts, Eva Lindh Waterworth,, Ulla-
Maija Pesola FL, Bente Christensen, Minna Mäkiniemi and Anne MacFarlane. Utilization of the
eHealth Implementation Toolkit: Identification of pilot services in Finland, Scotland, Sweden and
Norway. 2007 [cited 2013 20 October]; Available from:
http://www.ehealthservices.eu/instancedata/prime_product_julkaisu/npp/embeds/23411_e-
HIT_report_Final_ALL_PARTNERS.pdf.
9. Norway NCfTaUHoN. eHealth solutions across the Northern Periphery. 2013 [cited 2013 8
September]; Available from:
http://www.northernperiphery.eu/files/archive/Downloads/Project_Publications/11/Competitive%2
0Health%20Services%20brochure.pdf.
10. Natale Rd. Sink your teeth into dental care reform. 2011 [cited 2013 5 September];
Available from: http://www.abc.net.au/unleashed/3208234.html.
11. Goetzel RZ. Do Prevention Or Treatment Services Save Money? The Wrong Debate. 2012
[cited 2013 22 October]; Available from: http://content.healthaffairs.org/content/28/1/37.full.
12. Health USoP. Methodology: Models (taxonomy of HIA). Los Angeles2006 [cited 2013 27
September]; Available from: http://www.ph.ucla.edu/hs/health-impact/models.htm.
13. Sophia Schlette ML, Kerstin Blum. Integrated primary care in Germany: the road ahead.
International Journal of Integrated Care. 2009;9(14).
14. Tor Inge Romøren DOT, Brynjar Landmark. Promoting coordination in Norwegian health
care. International Journal of Integrated Care. 2011;11(Special 10th Anniversary Edition).
15. OECD. OECD Health Data 2013: How Does Norway Compare. 2013 [cited 2013 11 October];
Available from: http://www.oecd.org/norway/BriefingNoteNORWAY2012.pdf.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-21-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 22 of 23
16. Hanssen BH. The Coordination Reform: Proper treatment – at the right place and right time.
Norwegian Ministry of Health and Care Services; 2009 [cited 2013 11 September]; Available from:
http://www.regjeringen.no/upload/HOD/Dokumenter%20INFO/Samhandling%20engelsk_PDFS.pdf.
17. Organisation WH. The determinants of health. 2013 [cited 2013 13 September]; Available
from: http://www.who.int/hia/evidence/doh/en/
18. Policies EooHSa. Nordic Heath Care Systems: Recent Reforms and Current Policy Changes.
2009 [cited 2013 13 September]; Available from:
http://www.euro.who.int/__data/assets/pdf_file/0011/98417/E93429.pdf.
19. Katherine E Smith GF, Jeff Collin, Heide Weishaar, Anna B Gilmore. Is the increasing policy
use of Impact Assessment in Europe likely to undermine efforts to achieve healthy public policy? J
Epidemiol Community Health. 2010;64(6):478-87.
20. Dag Olaf Torjesen ABH. Cooperation and Coordination in Health Care. 2011 [cited 2013 9
September]; Available from:
https://conference.cbs.dk/index.php/nohr/health/paper/viewFile/999/449.
21. Services NMoHaC. The Coordination Reform: Proper treatment – at the right place and right
time. 2009 [cited 2013 8 September]; Available from:
http://www.regjeringen.no/upload/HOD/Samhandling%20engelsk_PDFS.pdf.
22. Prevention and Population Branch W, Integrated Care & Ageing Division of the Victorian
State Government, Department of Health, Australia. The determinants of health. 2011 [cited 2013
17 September]; Available from:
http://www.health.vic.gov.au/healthpromotion/what_is/determinants.htm.
23. Knut Rasmussen DB. Quality or equality? The Norwegian experience with medical
monopolies. 2007 [cited 2013 15 September]; Available from:
http://www.biomedcentral.com/1472-6963/7/20/table/T3.
24. Helsetilsyn S. Norwegian Board of Health Supervision. 2010 [cited 2013 20 September];
Available from: https://www.helsetilsynet.no/no/Norwegian-Board-of-Health-
Supervision/Organization/#countyorg.
25. Services MoHaC. The Coordination Reform. Oslo2008 [cited 2013 3 September]; Available
from: http://www.regjeringen.no/en/archive/Stoltenbergs-2nd-Government/ministry-of-health-
and-care-services/tema-og-redaksjonelt-innhold/kampanjesider/2008/the-coordination-
reform.html?id=524777.
26. Health TNIoP. The Norwegian Institute of Public Health. Oslo2013 [cited 2013 2 September];
Available from: http://www.fhi.no/eway/?pid=238.
27. Universitetssykehus O. Department of Ophthalmology Oslo2013 [cited 2013 2 September];
Available from: http://www.oslo-universitetssykehus.no/OMOSS/ENGLISH/ORGANISATIONAL-
UNITS/Sider/department-of-ophthalmology.aspx.
28. Norway I. Tromsø. 2013 [cited 2013 22 September]; Available from:
http://www.visitnorway.com/en/Where-to-go/North/Tromso/.
29. Kommune O. Senior Citizen's Community. Oslo2011 [cited 2013 22 September]; Available
from: http://www.oslo.kommune.no/english/health_/senior_citizens/.
30. Services MoHaC. Ministry of Health and Care Services. Oslo2012 [cited 2013 5 September];
Available from: http://www.regjeringen.no/en/dep/hod.html?id=421.
31. Harris P, Harris-Roxas, B., Harris, E., & Kemp, L. Health Impact Assesessment: A practical
guide. Sydney: Centre for Health Equity Training, Research and Evaluation, University of New South
Wales 2007.
32. Norway S. Minifacts about Norway 2013: Demographics, health and crime. 2013 [cited 2013
7 September]; Available from:
http://www.ssb.no/english/subjects/00/minifakta_en/en/main_03.html#tab0301.
33. Health NIoP. Health among the elderly (65 years and over) in Norway - fact sheet. 2013
[cited 2013 11 September]; Available from:](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-22-2048.jpg)
![PUBH6302-MA3-WYONE A/Prof Nick Higginbotham Wyiki Wyone c3156001
Page 23 of 23
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7630:1:0:0:::
0:0&MainContent_6894=6671:0:25,7646:1:0:0:::0:0&List_6673=6674:0:25,7658:1:0:0:::0:0.
34. Health NIoP. Smoking and smokeless tobacco in Norway - fact sheet. 2013 [cited 2013 11
September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7629:1:0:0:::
0:0&MainContent_6894=6671:0:25,7640:1:0:0:::0:0&List_6673=6674:0:25,7751:1:0:0:::0:0.
35. Health NIoP. Chronic pain prevalence in Norway – fact sheet. 2013 [cited 2013 9
September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7583:1:0:0:::
0:0&MainContent_6894=6671:0:25,7590:1:0:0:::0:0&List_6673=6674:0:25,7602:1:0:0:::0:0.
36. Health NIoP. Psychological problems and disorders in Norway - fact sheet. 2013 [cited 2013
9 September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7583:1:0:0:::
0:0&MainContent_6894=6671:0:25,7587:1:0:0:::0:0&List_6673=6674:0:25,7593:1:0:0:::0:0.
37. Health NIoP. Education level and health in Norway - fact sheet. Oslo2013 [cited 2013 9
September]; Available from:
http://www.fhi.no/eway/default.aspx?pid=240&trg=List_6673&Main_6664=6894:0:25,7630:1:0:0:::
0:0&MainContent_6894=6671:0:25,7643:1:0:0:::0:0&List_6673=6674:0:25,7649:1:0:0:::0:0.
38. Health-e-Solutions. Overview of Canada’s Health Care System. 2010 [cited 2013 5
September]; Available from: http://www.healthesolutions.ca/wp-content/uploads/2011/01/MB-
Overview-of-Canadas-Health-Care-systems.pdf.
39. Labor N. Right care Right place Right time. Sydney2011 [cited 2013 4 September]; Available
from:
http://www.parliament.nsw.gov.au/prod/web/common.nsf/cbe381f08171c2e8ca256fca007d6044/
365ca6edd5c453a5ca25788f00048421/$FILE/ATTG75Q2.pdf/Appendix%2012%20-
%20Right%20Care,%20Right%20Place,%20RightTime.pdf.
40. Improvement NIfIa. Quality and Service Improvement Tools: Reliable Design. 2012 [cited
2013 13 September]; Available from:
http://www.institute.nhs.uk/quality_and_service_improvement_tools/quality_and_service_improve
ment_tools/reliable_design.html.
41. Telemedicine NCfICa. The Norwegian Centre for Telemedicine. 2013 [cited 2013 20
October]; Available from: http://telemed.custompublish.com/about-nst.5108462-258955.html.
42. Telemedicine NCf. Innovation in e-Health and Telemedicine. 2013 [cited 2013 12 October];
Available from: http://www.ehealthservices.eu/project_partners/nst.
43. Systems HIaM. About HIMSS. Chicago2013 [cited 2013 5 October]; Available from:
http://www.himss.org/ASP/aboutHimssHome.asp.
44. Canada TCBo. Enhancing Interdisciplinary Collaboration in Primary Healthcare in Canada.
Ottawa2005 [cited 2013 28 October]; Available from:
http://www.eicp.ca/en/resources/pdfs/enhancing-interdisciplinary-collaboration-in-primary-health-
care-in-canada.pdf.
45. Physiotherapy TCSo. Public Health. London2012 [cited 2013 19 October]; Available from:
http://www.csp.org.uk/topics/public-health.](https://image.slidesharecdn.com/e607c7f0-e486-4e1d-8e8a-2eb311edb53d-160510102642/75/Health-Impact-Assessment-of-E-Medicine-and-Norway-s-Healthcare-Policy-Reform-23-2048.jpg)

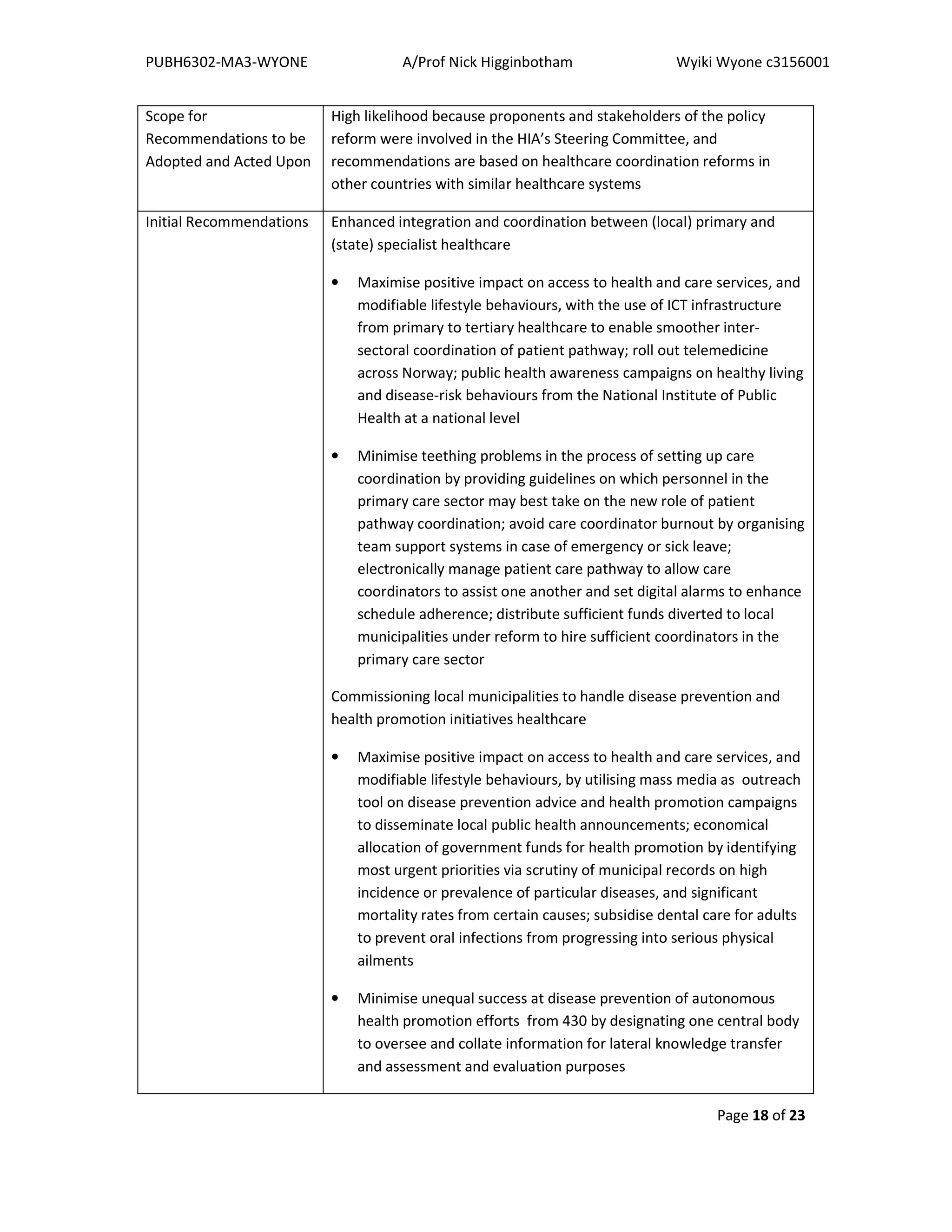
This document summarizes an equity-focused health impact assessment of Norway's 2012-2015 healthcare coordination reform. The reform aimed to decentralize services to local municipalities and improve coordination between primary, secondary, and tertiary care to enhance patient care pathways and disease prevention. An assessment was conducted to identify how the reform may positively or negatively impact population health and health equity. Key potential impacts identified included reduced waiting times and improved management of chronic diseases. Vulnerable groups like the elderly, disabled, and culturally diverse populations were most likely to benefit. The assessment provided recommendations to enhance benefits and mitigate risks to health equity.



































































