Download to read offline

























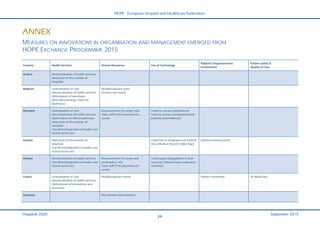
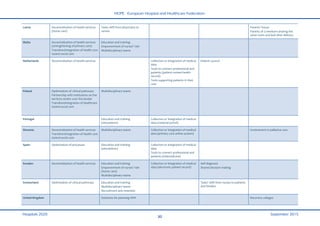


This document summarizes findings from the HOPE Exchange Programme on innovations in hospital and healthcare organization and management. Participants identified innovations in several areas across different European countries, including: centralizing care services; increasing home and community-based care; optimizing clinical pathways; empowering nurses' roles; implementing multidisciplinary care teams; and facilitating health data sharing and telemedicine. The document provides examples of specific innovations in various countries and discusses trends toward more patient-centered and integrated care models.


































































