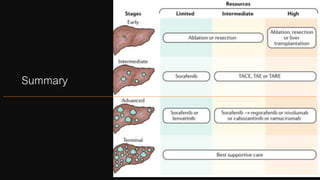
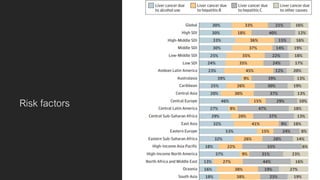
This document provides an overview of the management of hepatocellular carcinoma (HCC). It discusses the epidemiology, risk factors, diagnosis and staging, as well as treatment options for HCC. The major risk factors for HCC include hepatitis B virus, hepatitis C virus, and alcohol. Treatment depends on the stage and includes options such as liver transplantation, resection, ablation, transarterial chemoembolization, and the systemic therapy sorafenib. Prevention through vaccination and treating underlying liver diseases can help reduce cases of HCC.
![Epidemiology
• High incidence [>15 cases/100,000]
• East Asia
• Africa
• Intermediate incidence [3-15 cases/100,000
• Europe
• Southeast Asia
• Low incidence [<3 cases/100,000
• Americas
• Australia
5](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-5-320.jpg)
![Hepatitis B Disease Progression
Acute
Infection[1]
Chronic
Infection
Cirrhosis Death
5% to 10% of chronic HBV-
infected individuals[2,3]
Decompensation
20% to
30%[4]
> 90% of infected
children progress to
chronic disease (< 5%
of adults)[5]
23% of patients
decompensate within 5 yrs of
developing cirrhosis[3]
Liver
Cancer (HCC)
Liver
Transplantation
1. The elimination of hepatitis B. In: Buckley. Eliminating the public health problem of hepatitis B and C in the United States:
Phase One Report. 2016. 2. Iloeje. Liver Int. 2012;32:1333. 3. Fattovich. Hepatology. 1995;21:77. 4. Niederau. World J
Gastroenterol. 2014;20:11595. 5. Weinbaum. MMWR Recomm Rep. 2008;57:1. Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-8-320.jpg)
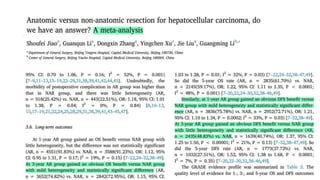
![Ethiopian Context
• HBV
• Overall pooled prevalence of 6%.
• HCC in TASH
• 51 patients, 2 years retrospective
• RFs: HBV and HCV: 48%; Alcohol : 45%
• HCC in referral clinic in Addis: Amir et al
• 46 patients with HCC, retrospective;
• RFs: 41% HBV, 45% HCV; 78% with Cirrhosis
• Management: TACE[16%], Sorafenib [18%], palliative care [31%].
9Sultan, Amir et al. “Liver Cancer in Ethiopia: Presentation, Prognosis, and Therapy: 1077.” The American Journal of Gastroenterology 114 (2019): n. pag.
Belyhun, Yeshambel et al. “Hepatitis viruses in Ethiopia: a systematic review and meta-analysis.” BMC infectious diseases vol. 16,1 761. 19 Dec. 2016,
doi:10.1186/s12879-016-2090-1](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-9-320.jpg)

![SURVIELLANCE RECOMMENDATION
• Patients with cirrhosis,
• Child-Pugh class A and B
• Child-Pugh class C, only if awaiting liver transplantation
• Noncirrhotic HBV with any of the following
• Active hepatitis (elevated serum alanine aminotransferase [ALT] and/or high viral load)
• Family history of HCC
• Africans and African Americans
• Asian males over 40 years of age
• Asian females over 50 years of age](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-12-320.jpg)

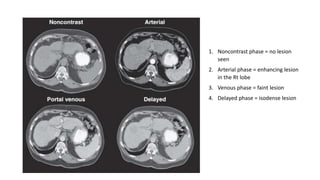
![Diagnosis
• Imaging with CT or MRI
• Classic arterial enhancement with venous wash out has Sn/Sp of 90/95%.
• AFP
• Is not specific.
• More helpful to detect recurrence
• Biopsy
• If nodule is atypical
• LR 4 and LR-M
• In noncirrhotic HCC [EASL Recommendation]
15](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-15-320.jpg)
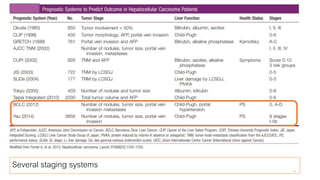
![Major Sources of Guidance/Guideline for Management of HCC
WEST
• Barcelona-Clínic Liver Cancer Staging
system (BCLC)
• American Association for Study of Liver
Diseases [AASLD]
• European Association for Study of Liver
[EASL]
• TNM [American Joint Committee on Cancer]
• The Cancer of the Liver Italian Program
(CLIP)
EAST
• The Hong-Kong Liver Cancer (HKLC)
• The Japan Integrated Staging (JIS)
• The Chinese University Prognostic Index
(CUPI)
• …
17](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-17-320.jpg)
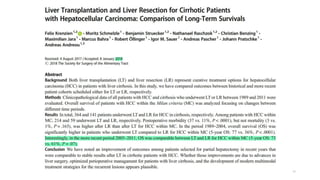
![Competing criteria for LT
• UCSF criteria also reported 75% survival.
• Mazzaferro then did large retrospective and
found 71% survival
• Tokyo [5 to 5 rule]: 5year OS 75%
• Many more…](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-25-320.jpg)


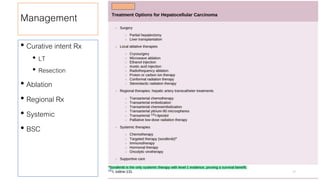
![Regional Therapies
• Transarterial Chemoembolization [TACE]
• First-line for unresectable, large/multifocal HCCs who do not have vascular invasion or extrahepatic spread.
• Patients at early stage in whom RFA is difficult to perform because of tumor location or medical
comorbidities
• For downstaging tumors that exceed LT Criteria.
• The objective response rate using enhancement criteria ranges between 58 and 86%.
• Transarterial radioembolization [TARE]
• ~40% objective tumor response rate with median survival of 15 months.
• The main indication is inoperable HCC.
41](https://image.slidesharecdn.com/hepatocellularcarcinoma2020-201018044359/85/Hepatocellular-carcinoma-2020-41-320.jpg)