Downloaded 33 times

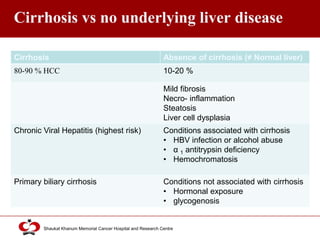





Hepatocellular carcinoma (HCC) is the most common type of liver cancer. Risk factors include cirrhosis of the liver caused by hepatitis B, hepatitis C, alcohol use, and non-alcoholic fatty liver disease. Screening high-risk patients allows early detection when treatment is most effective. HCC incidence varies globally and is increasing due to risk factor epidemics.