Normal Hemostasis
Normal Hemostasis
Sequenceof events following vascular injury
1. Arteriolar vasoconstriction (transient effect)
Reflex neurogenic mechanism
Local secretion of endothelin
2. Primary hemostasis – PLATELET
- Damage to the endothelium exposes platelets to the subendothelial
extracellular matrix (ECM).
- Platelets adhere to the ECM and become activated (Activation)
a. Shape Change
b. Release granules
c. Recruit other platelets to site (Aggregation)
- Form a HEMOSTATIC plug
5.
Normal Hemostasis
Normal Hemostasis
3.Secondary Hemostasis - COAGULATION
a. Tissue factor, a membrane-bound procoagulant factor synthesized by
endothelium is exposed at the site of injury. It acts in conjunction with the
material secreted by platelets to activate the coagulation cascade.
b. Phospholipid complex expression
c. Thrombin activation
a. Formation of thrombin induces more platelet recruitment and granule
release
d. Fibrin Polymerization – resulting in local fibrin admixed with platelets –
form plug to prevent further hemorrhage.
4. Antithrombotic Counter-Regulation
a. Release of components to limit the size of hemostatic plug
6.
Role of Endothelium
Roleof Endothelium
• Both Antithromotic properties & Prothrombotic
Properties.
• Antithrombotic (Anticoagulant) Properties of Endothelial Cells
– Antiplatelet
– 1. Barrier to subendothelial collagen - prevent
platelets and plasma factors from exposure
– 2. Prostacyclin - PGI2 , and Nitric Oxide - inhibit
platelet adhesion and aggregation
– 3. Express adenosine diphosphatase to degrade ADP
(ADP promotes platelet aggregation)
7.
Antithrombotic (Anticoagulant) Propertiesof Endothelial
Antithrombotic (Anticoagulant) Properties of Endothelial
Cells cont……..
Cells cont……..
• Anticoagulant properties
• 1. Membrane associated, heparin-like molecules
• 2. Thrombomodulin - specific thrombin receptor
• -Binds to thrombin making it an anticoagulant which can activate
protein C - activeProtein C - inhibits clotting by cleaving factors Va
and VIIIa Requires protein S - synthesized by endothelial cells
• 3. Synthesizes tissue factor pathway inhibitor – complexes and
inhibits Factors VIIa and Xa
• 4. Plasminogen activators which promote fibrinolytic activity to
clear fibrin deposits from endothelium
8.
Prothrombotic (Procoagulant) Propertiesof
Endothelial cells
• Endothelial cells may be activated by infectious agents,
hemodynamic factors, plasma mediators and cytokines or
injured indirectly.
• 1. Synthesize, store, and release von Willebrand factor (vWF) - essential
cofactor for platelet binding to collagen and other surfaces. Stored in
Weibel-Palade bodies.
• 2. Endothelial cells are also induced by cytokines (eg: TNF, or IL-1) or
bacterial endotoxin – to secrete tissue factor (Factor VII) which activates
the extrinsic clotting pathway.
• 3. Endothelial cells bind IXa and Xa and increase their catalytic activities
• 4. Secrete plasminogen activator inhibitors - to depress fibrinolysis
9.
Role of Platelets
Roleof Platelets
• Play a central role
• Round, smooth discs with glycoprotein receptors
• Two types of granules
– Alpha granules: Fibrinogen, fibronectin, V, VIII,
PDGF & TGF
– Dense granules (Delta granules): ADP & ATP, Ca,
Histamine, Serotonine & Epinephrine
10.
Role of Platelets
Roleof Platelets
• Three reactions: 1. Adhesion & shape change
mediated via interaction with vWF. 2. Secretion i.
e. release reaction. 3. Aggregation:ADP + TxA2
start reaction which leads to enlarging platelet
aggregation Primary hemostatic plug
• Activates coagulation generated thrombin increasing
aggregation Platelet contraction - fused mass of platelets,
fibrin formed cements mass Secondary hemostatic plug.
11.
Coagulation cascade
Coagulation cascade
Aclot is formed by an enzymatic cascade = series of zymogen
activations in which an activated form of one coagulation factor
catalyses the activation of the next.
Reaction Complex is composed of an enzyme - activated coagulation
factor + a substrate - proenzyme -coagulation factor which are
assembled on a phospholipid complex and held together by calcium
ions.
The coagulation cascade is usually divided into extrinsic and intrinsic
pathways which converge where factor X is activated. However, this
division is an artifact of in vitro testing. Several interconnections occur
between the two pathways.
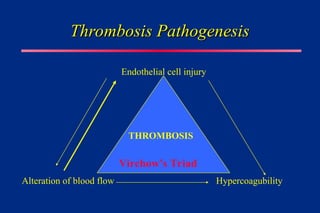
Endothelial cell injury
Endothelialcell injury
• Dominant feature. Lead to thrombosis by itself.
• Exposes subendothelial ECM – Platelet adhesion
--- Release of tissue factors ----- Depletion of
prostacyclin ------ Primary & secondary
hemostatic plug formation
15.
Causes of endothelialinjury causing
Causes of endothelial injury causing
thrombosis
thrombosis
• Endocardial injury in M.I.
• Ulceration of Atheromatous plaque
• Trauma to vascular endothelium
• Inflammatory vascular injury as in case of vasculitis
• Bacterial endotoxins
• Dysfunction of endothelium as in hemodynamic stress of
hypertension or turbulent flow over scarred valves
• Homocystinuria, Products of cigarette smoke,
hypercholestremia, radiation injury
16.
Alteration in NormalBlood Flow
Alteration in Normal Blood Flow
• Normal Blood flow – Laminar or Axial
Formed elements
Plasma
17.
Alteration in NormalBlood Flow
Alteration in Normal Blood Flow
• Disrupt normal laminar flow:
– Allows platelets to contact endothelium
– Prevents dilution of activated clotting factors by fresh-flowing
blood
– Allows the build up of thrombi (slows the inflow of
anticoagulants)
– Promotes endothelial cell activation
18.
Causes where disruptedblood flow
Causes where disrupted blood flow
leads to thrombosis
leads to thrombosis
• Ulcerated atherosclerotic plaque leads to turbulence ----
thrombosis
• Aneurysms cause local stasis ----- thrombosis
• M.I. --- Noncontractile myocardium ---- stasis ---
thrombosis
• Mitral stenosis --- stasis or turbulence – thrombosis
• Hyperviscosity syndromes like Polycythemia --- small
vesels stasis --- thrombosis
• Sickle cell disease --- small vessel stasis --- thrombosis
19.
Hypercoaguability
• Definition: anyalteration of the coagulation pathways
that predisposes to thombosis
• Primary or Secondary
– Defect in Coagulation factors
– Defect in Inhibitory factors
20.
Hypercoaguability
• Primary (Genetic)
•Mutation in factor V gene
(Factor V Leiden)
• Prothrombin gene
• Methyltetrahydrofoalte
gene
• Antithrombin III defi.
• Protein C defi.
• Protein S defi.
• Secondary (Acquired)
• Immobilisation
• M.I. & A.Fibrillation
• Cancer
• Heparin induced
throbocytopenia
• Anti phospholipid Ab
• Oral contraceptives
21.
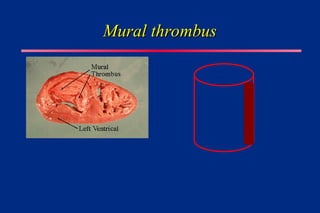
TERMINOLOGY AND MORPHOLOGY
(Relatedto Thrombosis)
THROMBOSIS: Formation, development or presence of a
solid mass within the blood vessels or heart. Adherent to the
vascular endothelium and must be differentiated from a
simple (post mortem) blood clot.
THROMBUS: An aggregation of blood factors, primarily
platelets and fibrin with entrapment of cellular elements,
frequently causes vascular obstruction at the point of its
formation or embolism
22.
TERMINOLOGY AND MORPHOLOGY
(Relatedto Thrombosis)
THROMBI: Pleural of thrombus ie: several aggregations
within the blood vascular system.Thrombi may develop
anywhere in cardiovascular system: Cardiac chambers,
Valves, Arteries (usually endothelial injury), Veins (often a
result of stasis), Capillaries
Arterial thrombi are attached and grow away from the heart.
Venous thrombi are attached and grow in the direction of
blood flow (to heart).
Arterial and venous thrombi differ!
23.
ARTERIAL Thrombi
• Generallydue to endothelial injury, initial thrombus is
composed of aggregated platelets and RBC's and is soft,
friable and red.
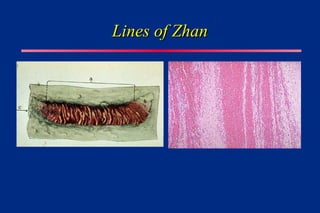
• As arterial thrombi grow, flow patterns adjacent to the
thrombi cause fibrin to be deposited and the platelet mass
that persists is transformed into a fibrin mass. Fibrin
strands polymerize between the separating and
degenerating platelets. The alternating lines of yellow
platelets and fibrin separating RBC's forms the lines of
Zahn.
VENOUS Thrombi or
Phlebothrombosis
•A venous thrombi is composed of fibrin strands with entrapped
RBC's, since the dominant mechanism of formation is coagulation.
• Almost invariably occlusive
• Create a long cast in venous lumen
• Form in static environment so contain more RBCs. Also called as
RED OR STASIS THROMBI
• 90% ARE IN VEINS OF LOWER EXTREMETIES
• Other sites: Upper extremities, periprostatic plexus, periuterine
plexus & periovarian plexus, dural sinuses, portal vein, hepatic vein
28.
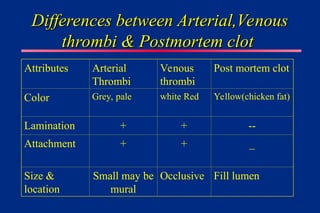
Differences between Arterial,Venous
Differencesbetween Arterial,Venous
thrombi & Postmortem clot
thrombi & Postmortem clot
Attributes Arterial
Thrombi
Venous
thrombi
Post mortem clot
Color Grey, pale white Red Yellow(chicken fat)
Lamination + + --
Attachment + + _
Size &
location
Small may be
mural
Occlusive Fill lumen
29.
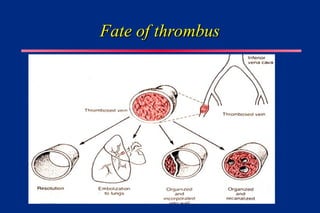
OUTCOME OF THROMBIor Fate
• 1. Lysis of thrombus (due to potent thrombolytic/ fibrinolytic
activity of blood)
• 2. Propagation of a thrombus ( in size) - may eventually
obstruct the vessel
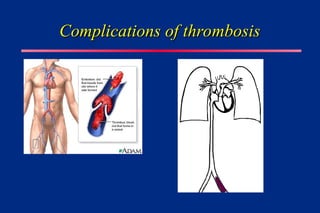
• 3. Embolization - possible
• 4. Organization - The presence of a thrombus stimulates
reaction which will result in inflammation and fibrosis.
Smooth muscle cells and fibroblasts will proliferate and
invade. The thrombus will become firm and grey-white. and
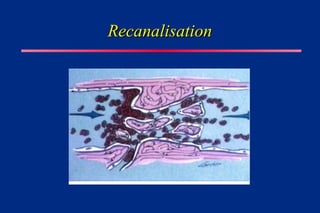
• Recanalization - New lumina, lined by endothelial cells form to
allow blood flow through the damaged vasculature
Infarction
Infarction
• DEFINITION: Areaof ischemic necrosis caused by
occlusion of either the arterial supply or the venous
drainage in a particular tissue.
• Examples of infarction we see commonly: M.I.,
Pulmonary Infarction, Bowel infarction, Gangrene
35.
Infarction Pathogenesis
Infarction Pathogenesis
•99% are due to thrombotic or embolic events &
almost are due to occlusion of arteries.
• Other: 1. Local vasospasm 2. Expansion of
atheroma 3. Extrinsic compression by tumor 4.
Twisting of vessels (Testicular torsion or
volvulus) 5. Compression of vessels by edema 6.
Traumatic rupture 7. Strangulation in hernia 8.
Cardiogenic shock
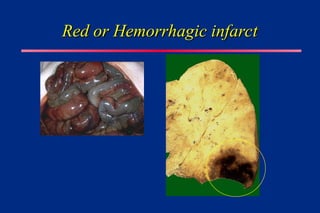
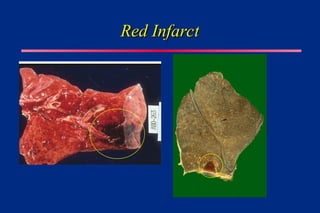
Red or HemorrhagicInfarcts
Red or Hemorrhagic Infarcts
1. With venous occlusion as in case of ovarian torsion
2. In loose tissue as in lung which allows blood to collect
in infarcted area
3. Tissues with dual blood supply e.g. lung & intestine
4. Tissues that were previously congested due to
obstructed venous flow
5. When the flow is reestablished to the site of infarction
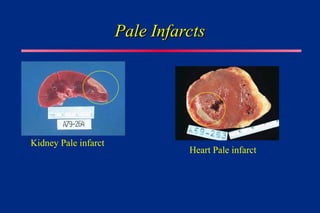
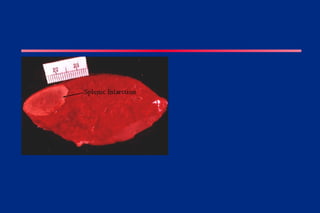
White or AnemicInfarcts
White or Anemic Infarcts
1. Arterial occlusion
2. Solid organs
3. Organs with end arterial blood supply
4. Heart, Spleen & kidneys
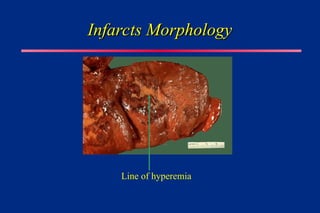
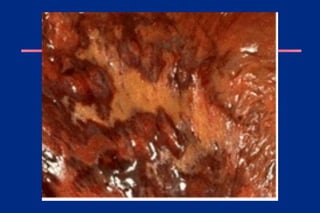
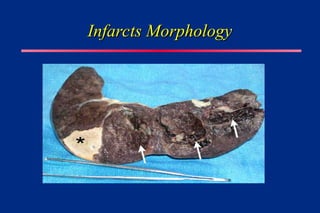
Infarcts Morphology
Infarcts Morphology
•Typically WEDGE shaped with occluded vessel at the
apex & the periphery of the organ forming base.
• Lateral margins irregular
• If the base is formed by serosal surface FIBRINOUS
EXUDATE can be seen.
• All infarcts are poorly defined & hemmorrhagic to begin
with.
• With the time margins show a narrow rim of hyperemia
due to inflammation at the edge.
Infarct -morphology
Infarct -morphology
•White infarcts with the time become more
progressively Pale & are sharply defined.
• In spongy organs hemorrhage is too extensive &
lesion never gets pale. However it gets more firm
& brown due to hemosiderin pigment.
48.
Infarct - Microscopy
Infarct- Microscopy
• Up-to 12 to 18 hrs.: No change except
hemorrhage
• Within few inflammatory response at the margins.
• Ischemic coagulative necrosis except in Brain,
where liquefactive necrosis is seen.
• In solid organs infarcts are healed by scar.
• Septic infarcts form abscess.
49.
Major determinants ofinfarct
Major determinants of infarct
development
development
• Dependent upon
• 1. Degree/severity of injury to vascular supply
• 2. Size of artery affected
• 3. Degree of vascular occlusion
• 4. Collateral blood supply available
• 5. Vulnerability of cells to ischemia
• 6. O2 carrying capacity of RBC's at time of infarct
50.
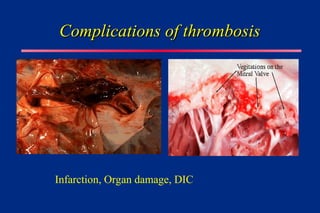
Complications of Infarction
Complicationsof Infarction
• Embolism
• Death
• Serosal fibrinous inflammation
• Dysfunction of the organ
• Abscess formation
• Gangrenous change