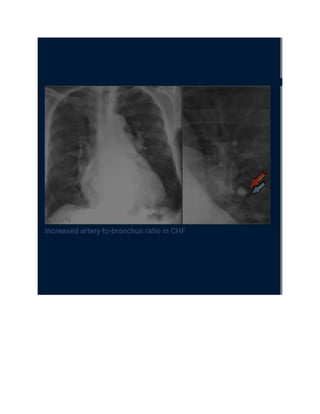
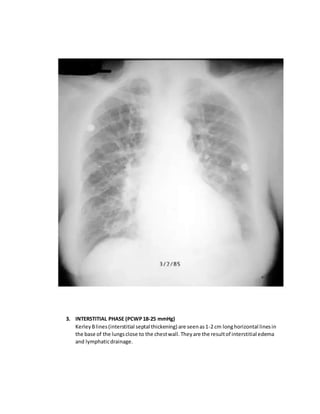
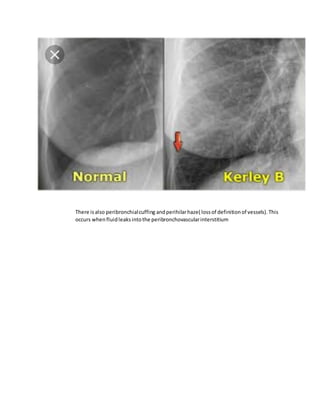
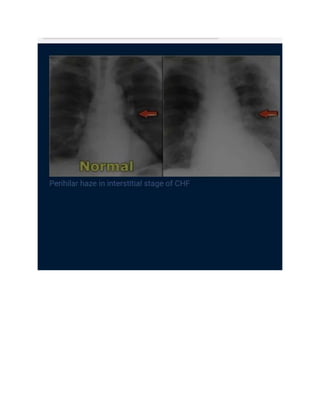
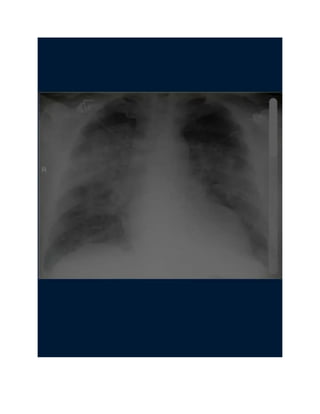
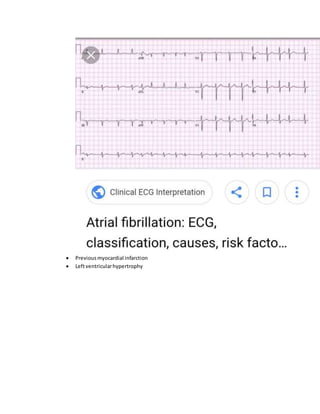
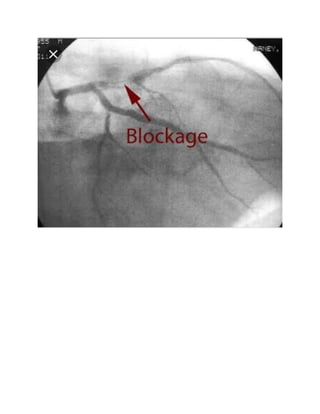
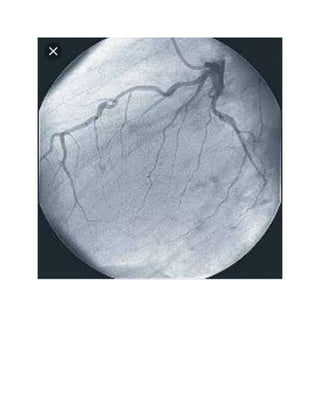
This document provides information on heart failure including definitions, classifications, etiologies, pathophysiology, clinical features, and investigations including radiology. Heart failure is defined as the inability of the heart to pump blood sufficiently to meet metabolic demands. It is classified in various ways including reduced vs preserved ejection fraction. Causes include ischemic heart disease, hypertension, cardiomyopathy, and arrhythmias. Radiography findings in congestive heart failure progression include enlarged cardiac silhouette, vascular redistribution of blood flow, and eventual interstitial edema. Echocardiography is useful for assessing ventricular function, valves, pressures, and detecting structural abnormalities.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















