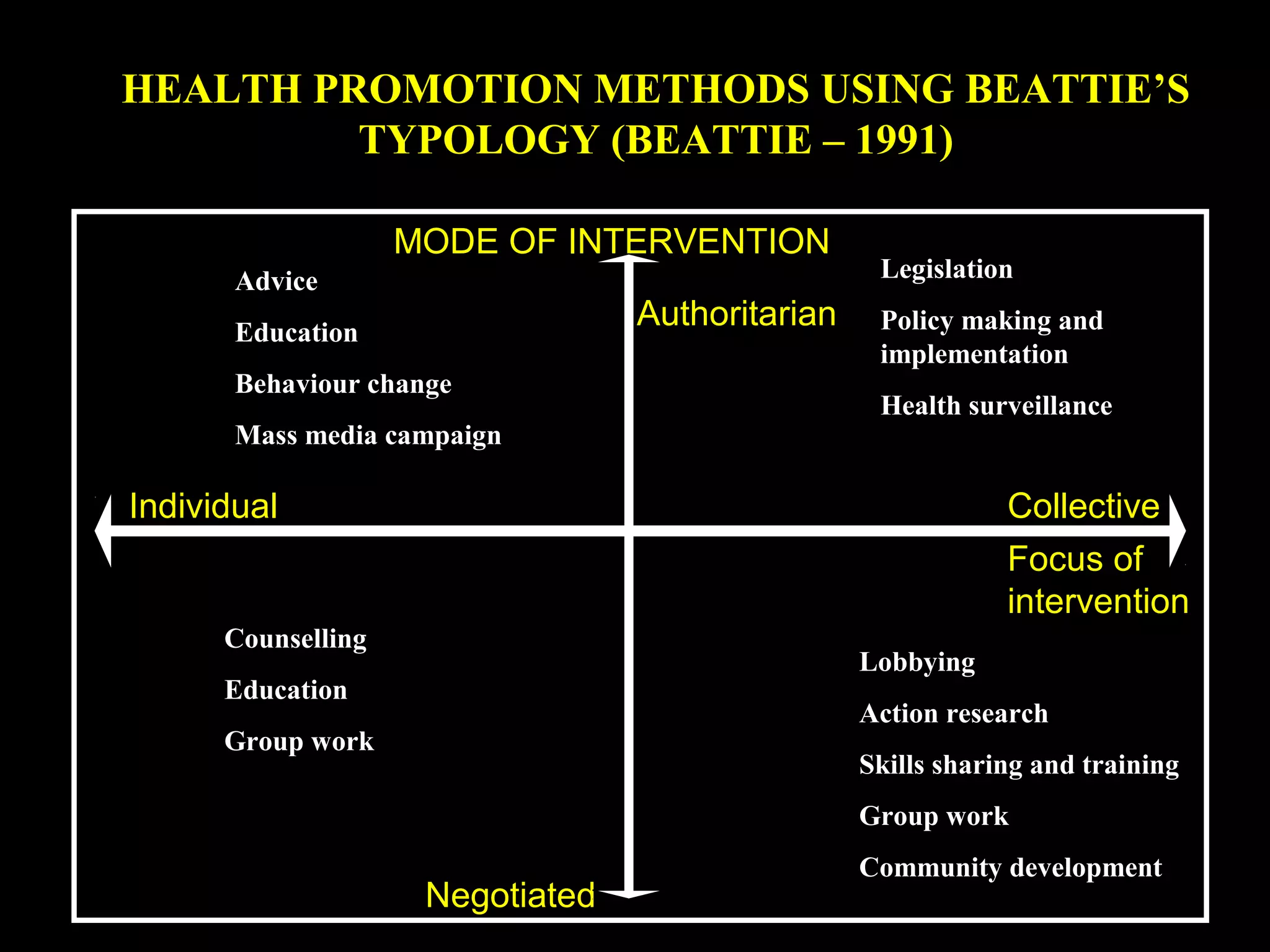
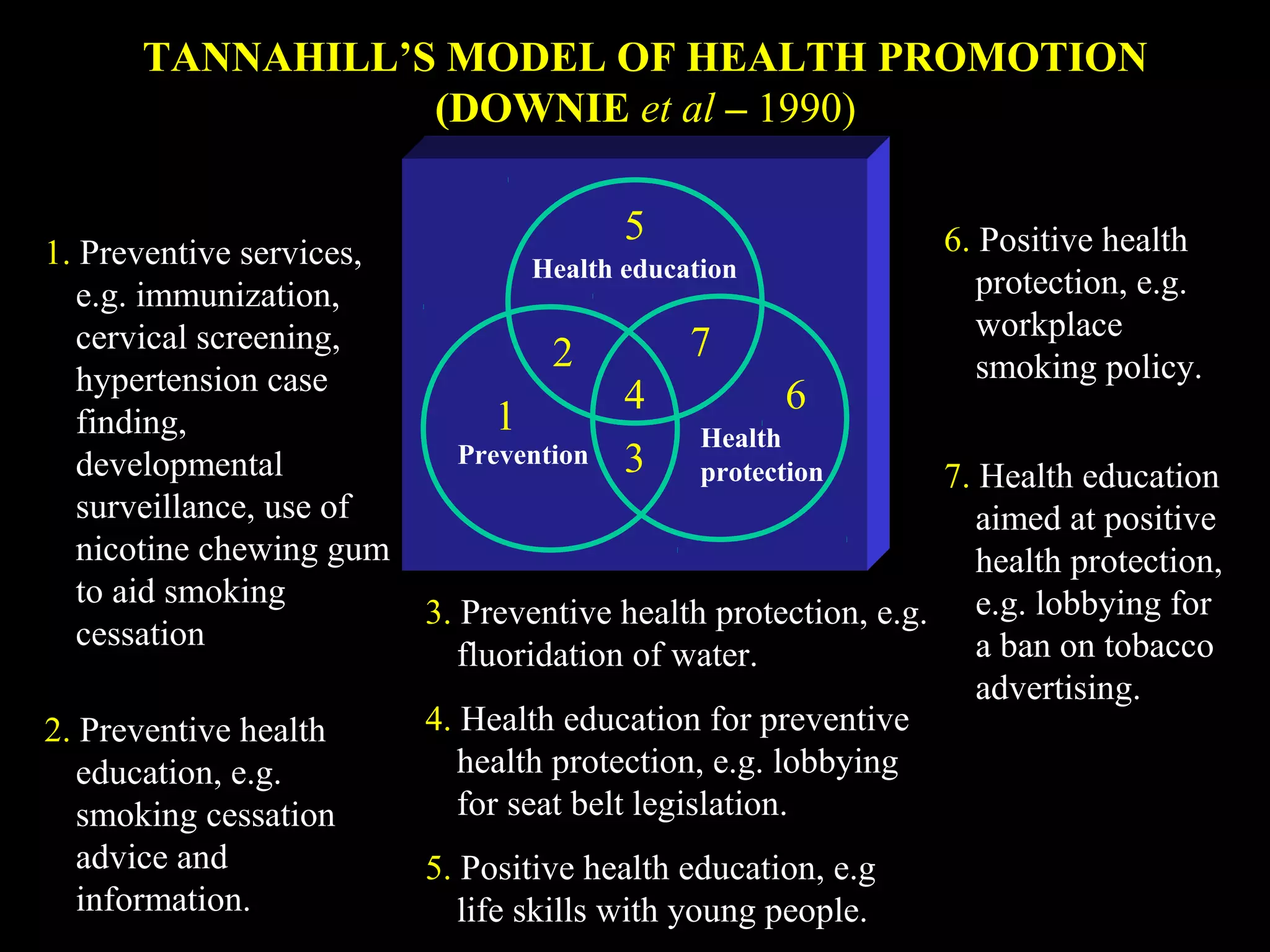
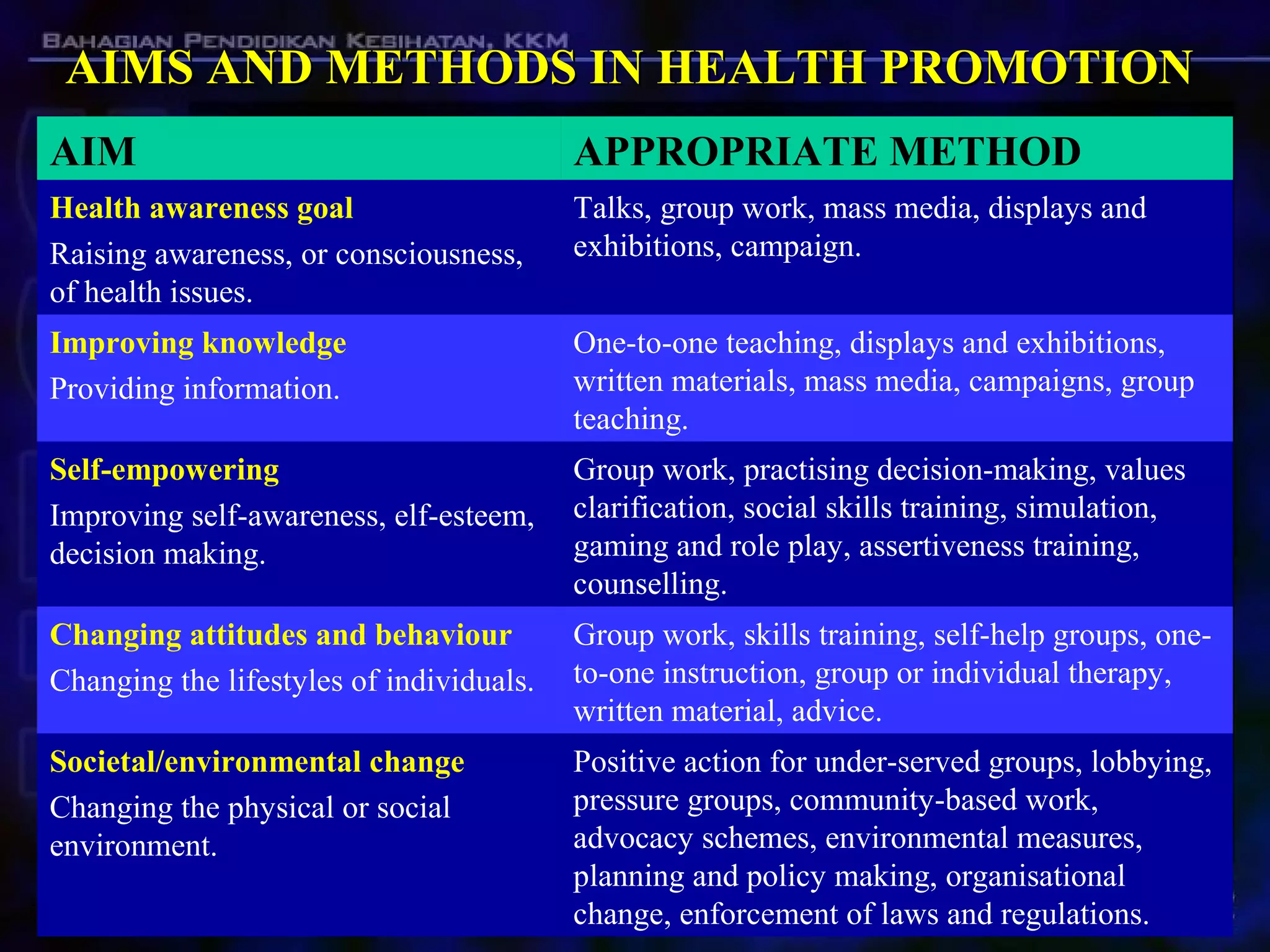
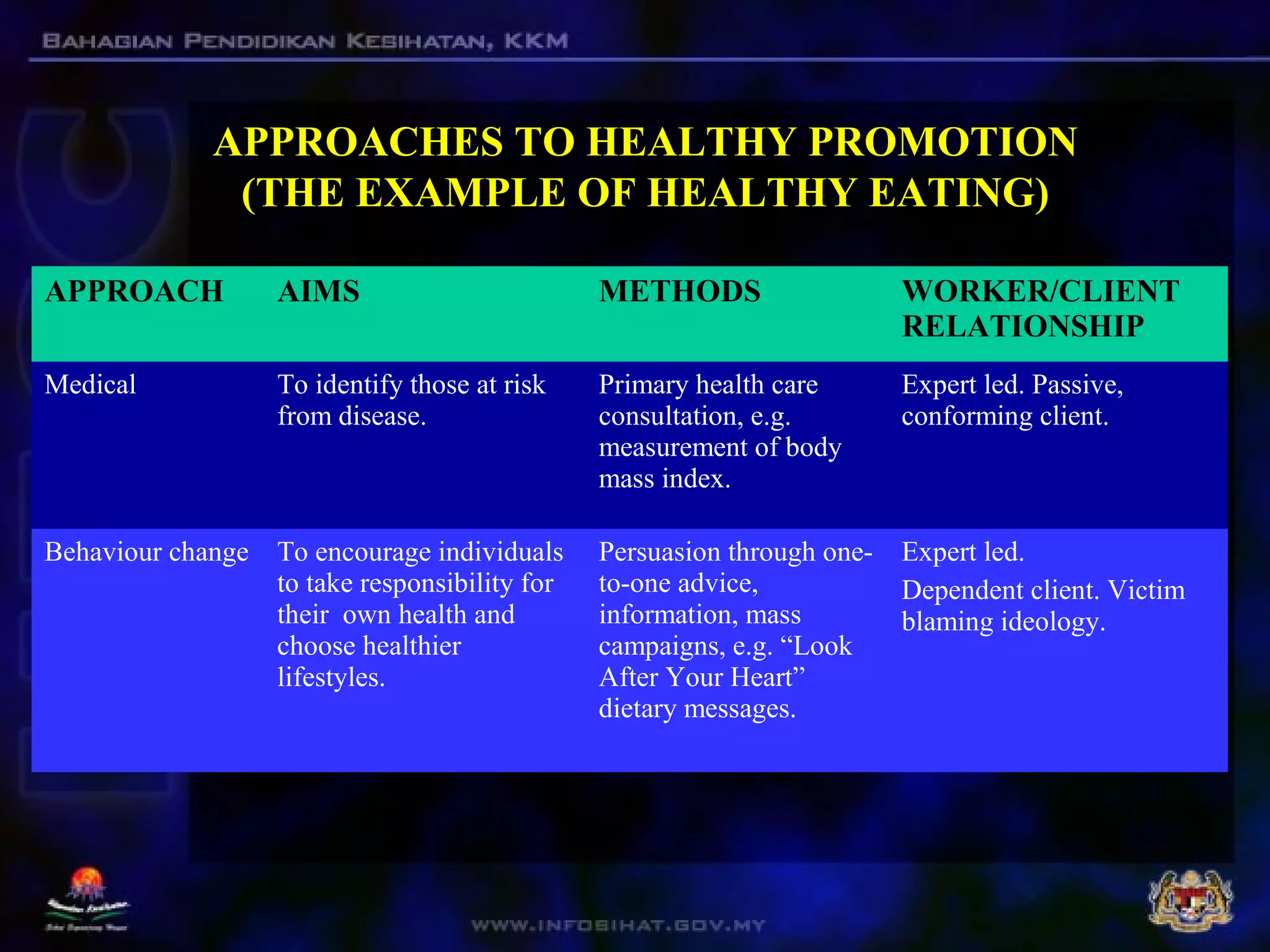
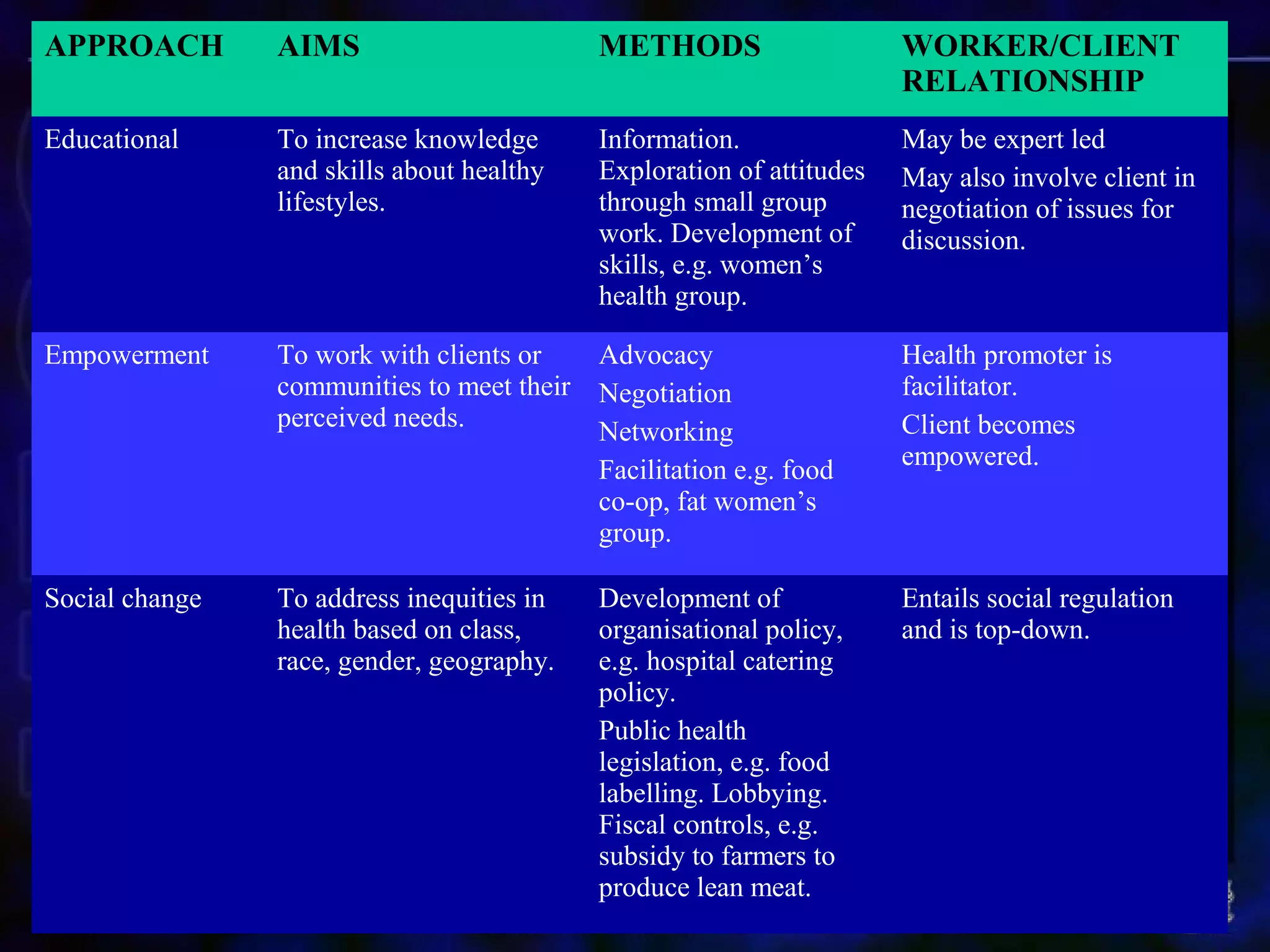
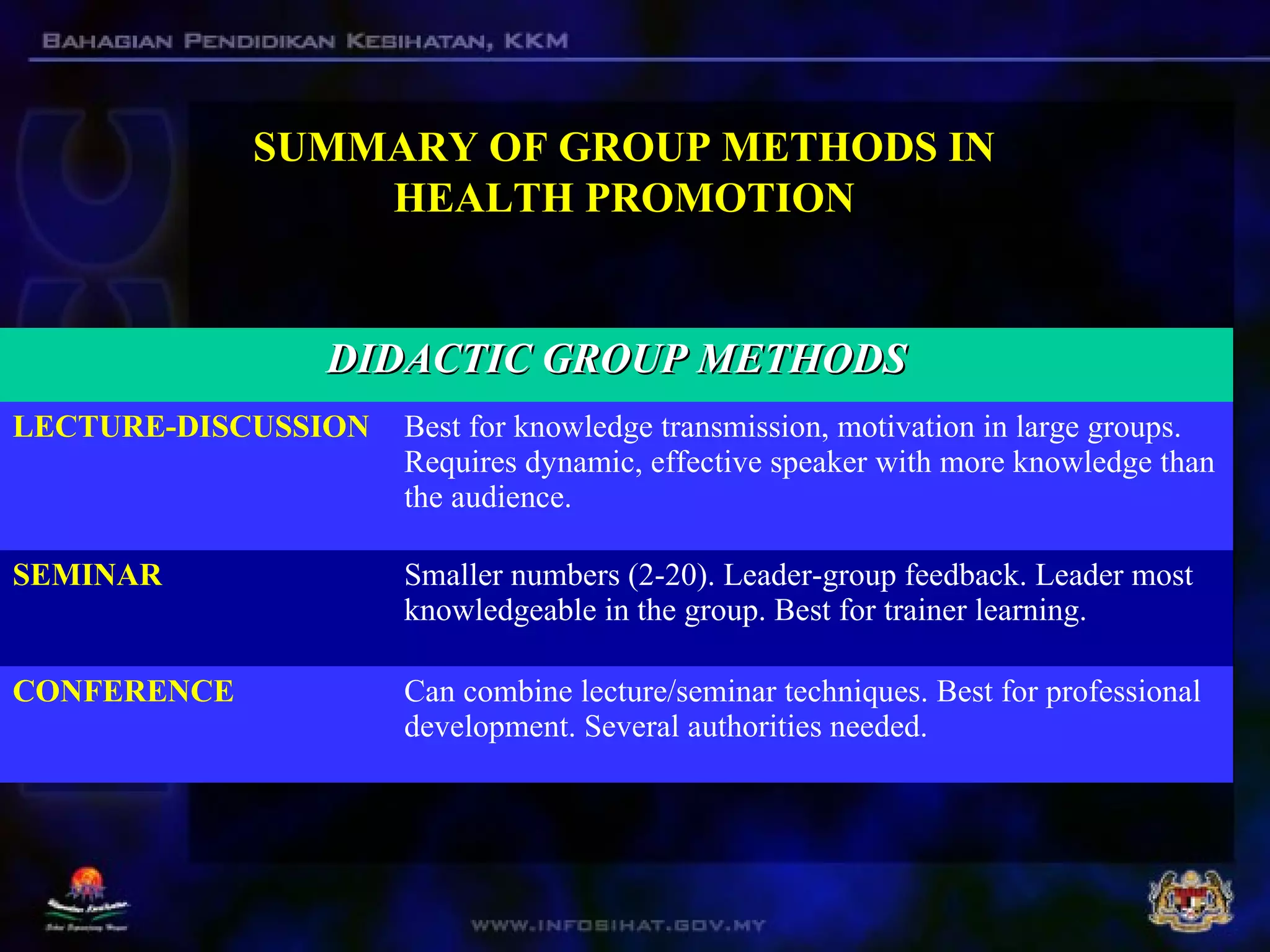
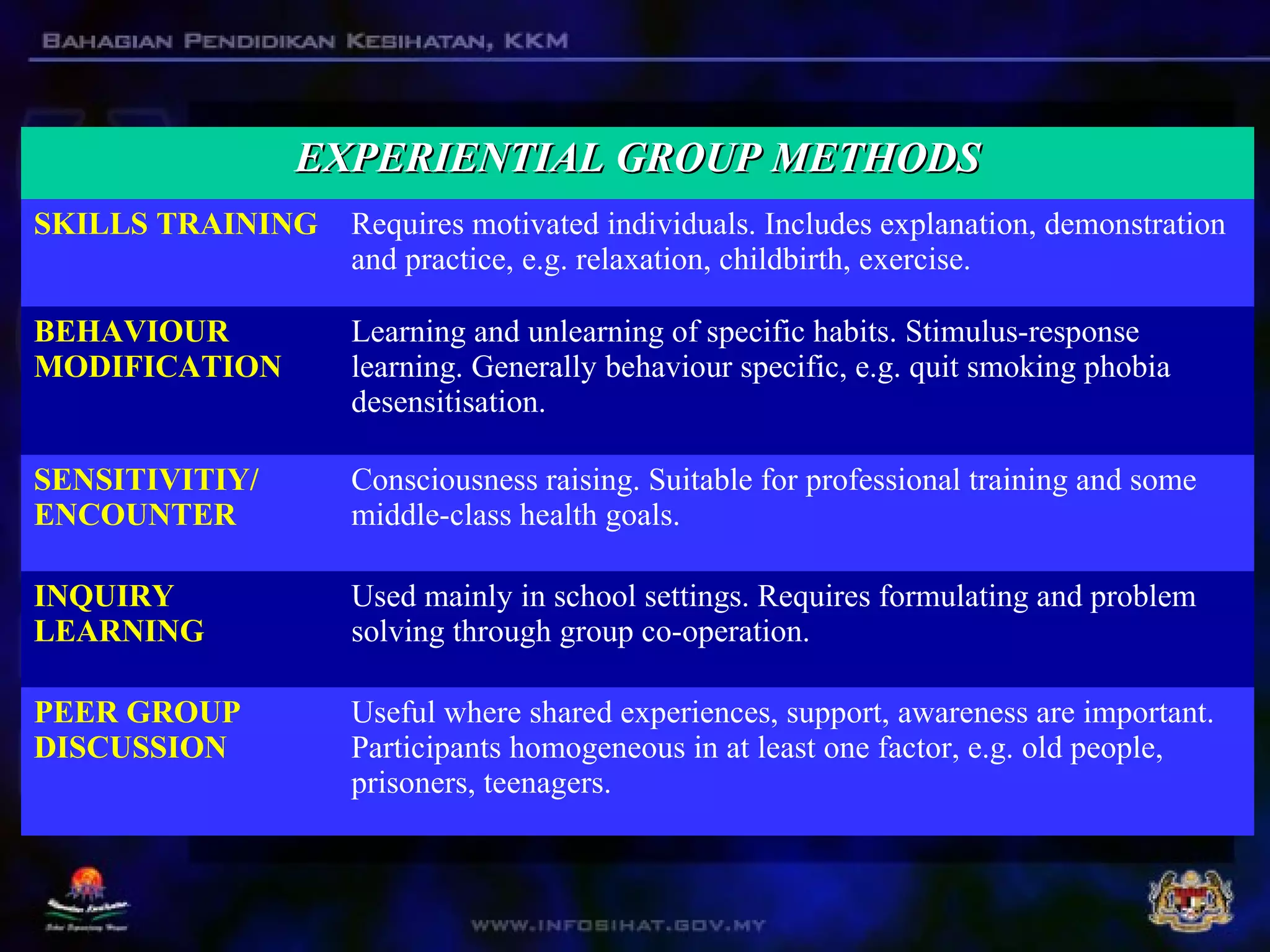
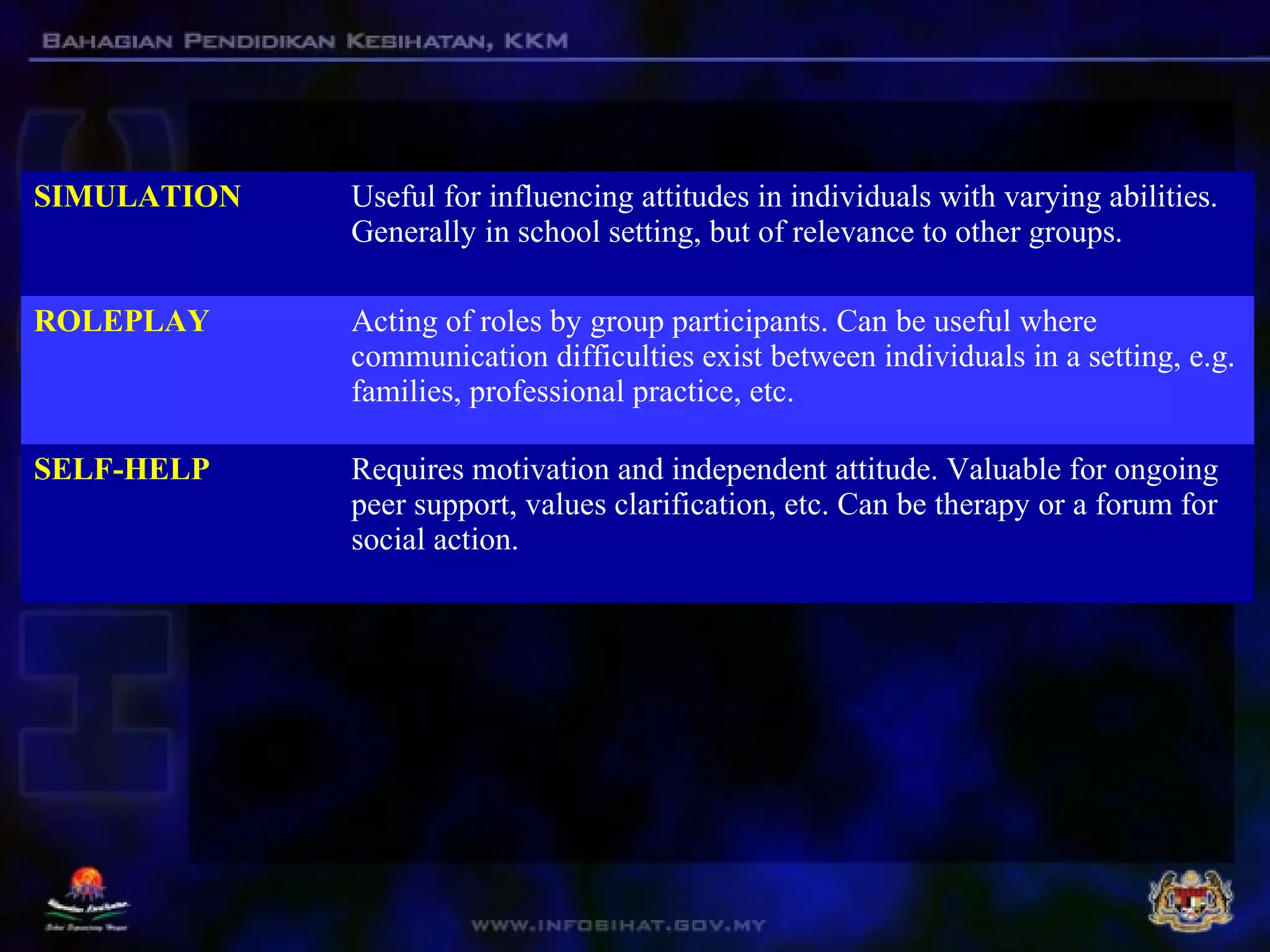
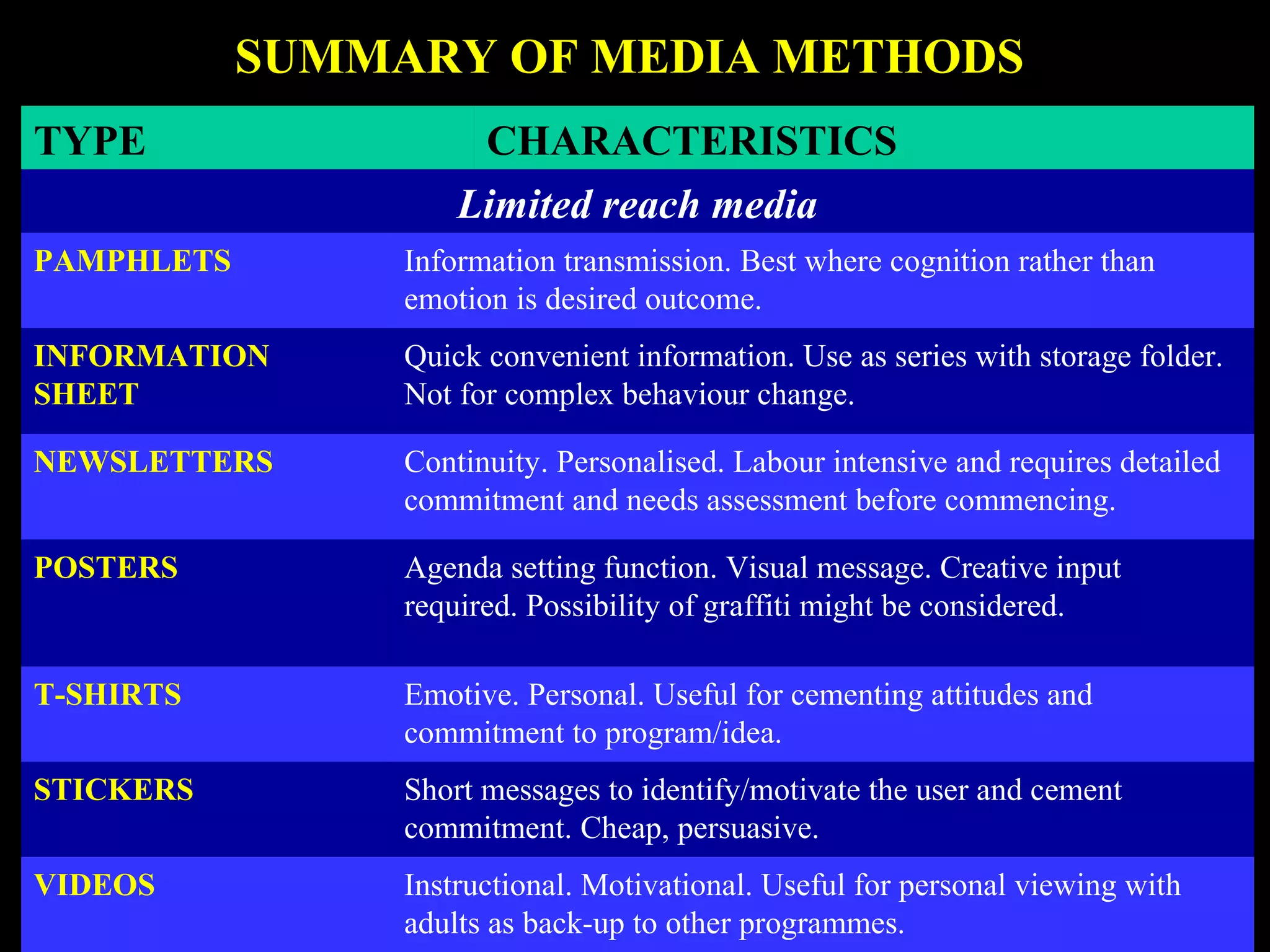
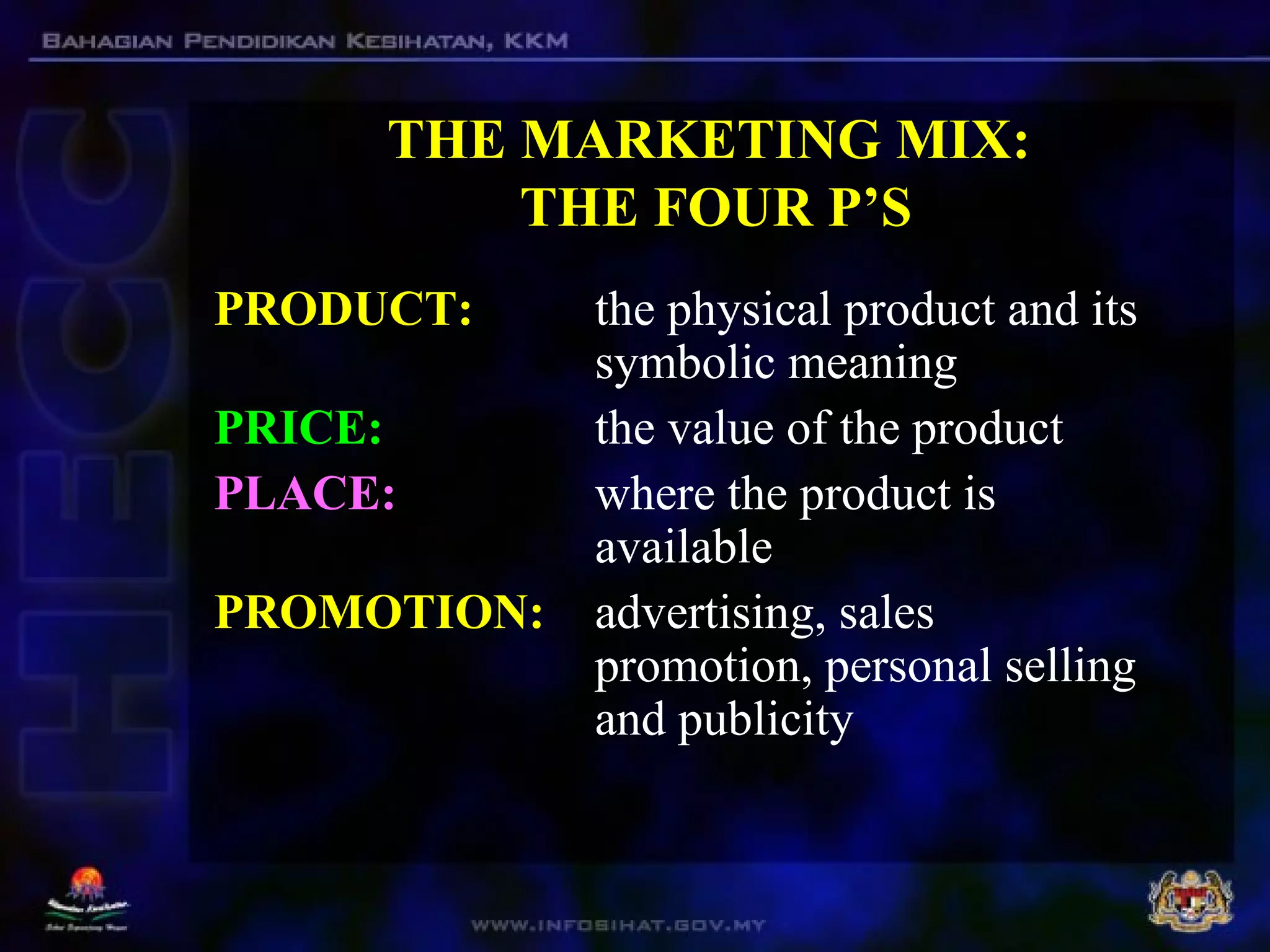
The document outlines various approaches to health promotion, including medical, behavior change, educational, empowerment, and societal change methodologies. It discusses intervention activities utilized in health promotion, emphasizing the importance of selecting appropriate methods based on sound rationale and target populations. Additionally, it highlights both individual and group approaches, as well as the role of mass media in influencing health behaviors and promoting public awareness.

















![health promotion lecture notes 2023[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/healthpromotionlecturenotes2023autosaved-240524204053-9ab2f7a0-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































