Downloaded 203 times

![• According to Stening BP below 90 mm Hg persisting for more
than 60 minutes in acute subdural hematoma was strong
predictor of bad outcome.
• White et al found that in pediatric trauma odds of survival
increased 19-fold when maximum systolic blood pressure was
greater or equal to 135 mm Hg
Stening WA, Berry Q, Dan N G, et al. Experience with acute subdural
hematomas in New South Wales. Austral NZ] Surg 1986;56:549—56.
White JR, Farukhi Z, Bull C, Christensen J, Gordon T, Paidas C,
Nichols DG. Predictors of outcome in severely head-injured
children. Crit Care Med 2001 ;29(3):534—40](https://image.slidesharecdn.com/headinjuryassesment-160619134220/85/Head-injury-assesment-11-320.jpg)
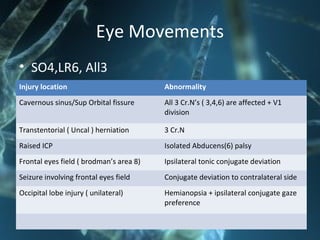
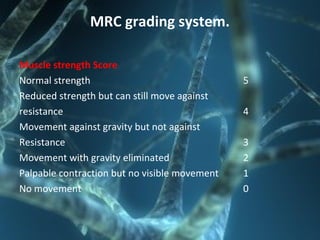
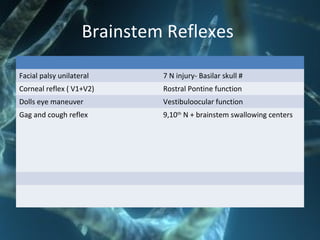
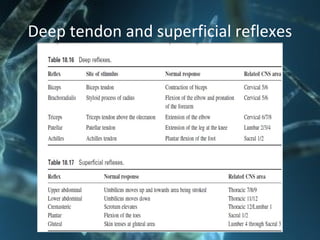
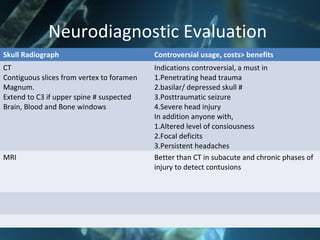
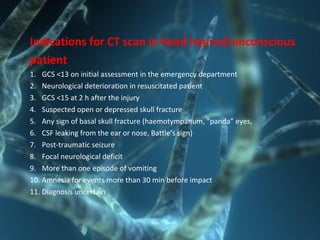


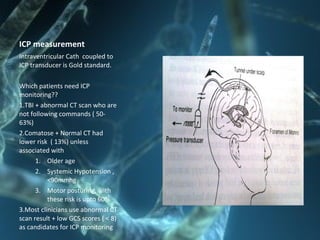

The document provides guidance on assessing patients with head injuries. It discusses performing a thorough neurological exam to establish a baseline and monitor for changes. The exam includes assessing level of consciousness, pupil size and reactivity, eye movements, motor function, reflexes, and involuntary movements. Vital signs, history of the injury, and signs of base of skull fractures are also important to evaluate. Repeated assessments are needed to monitor for deterioration. CT scan is recommended for severe head injuries or clinical worsening to identify brain injuries requiring intervention.




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















