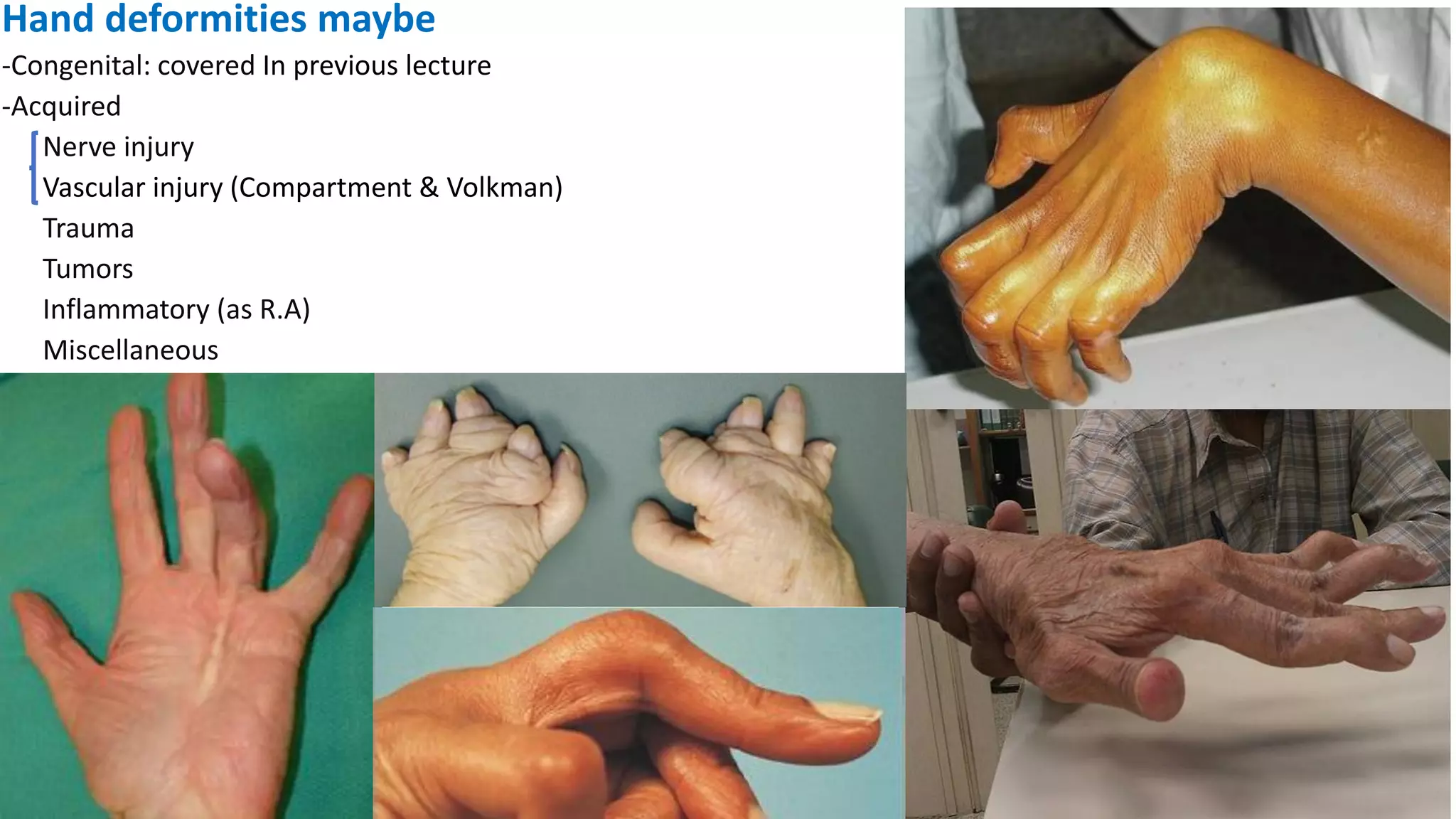
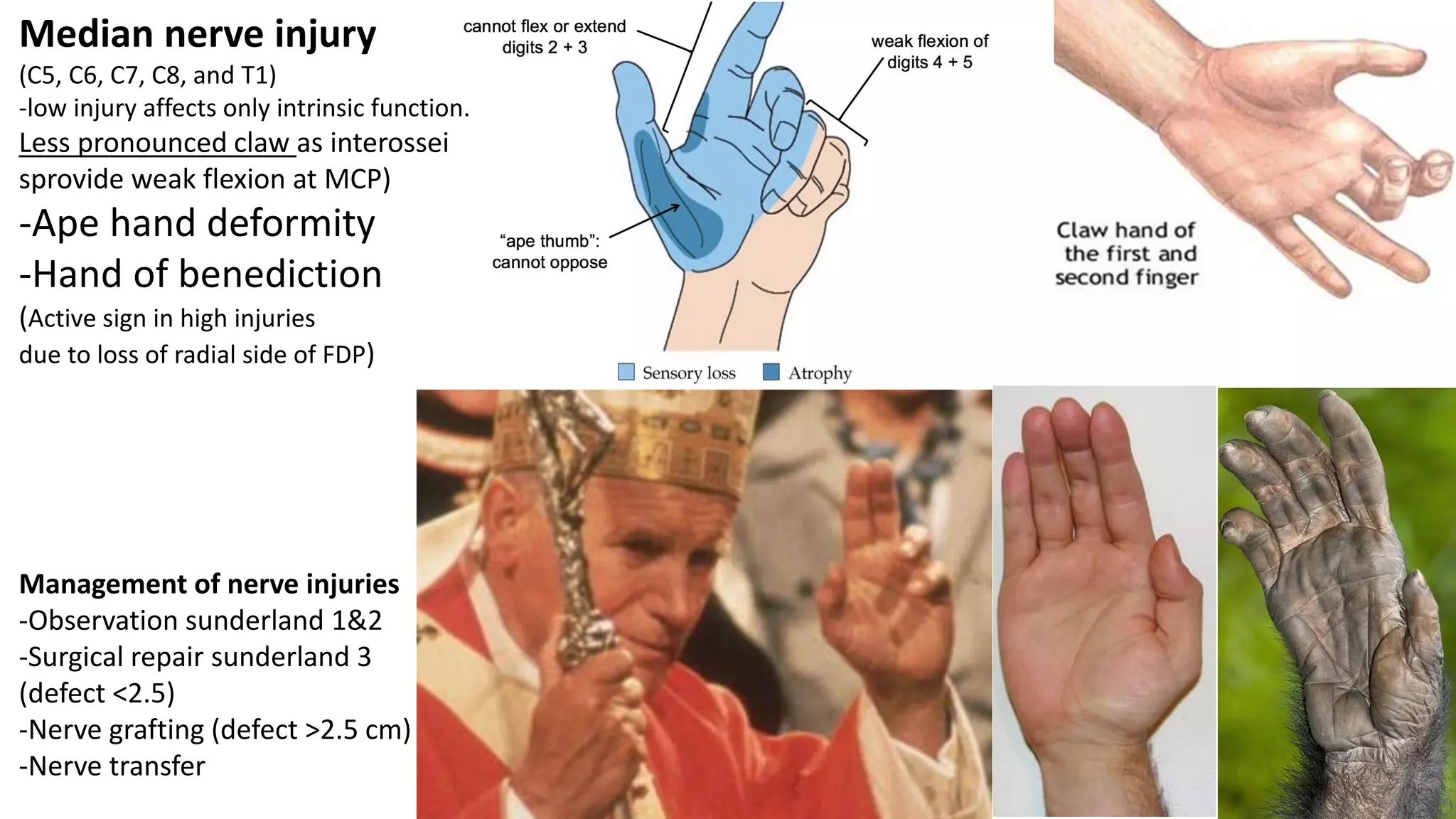
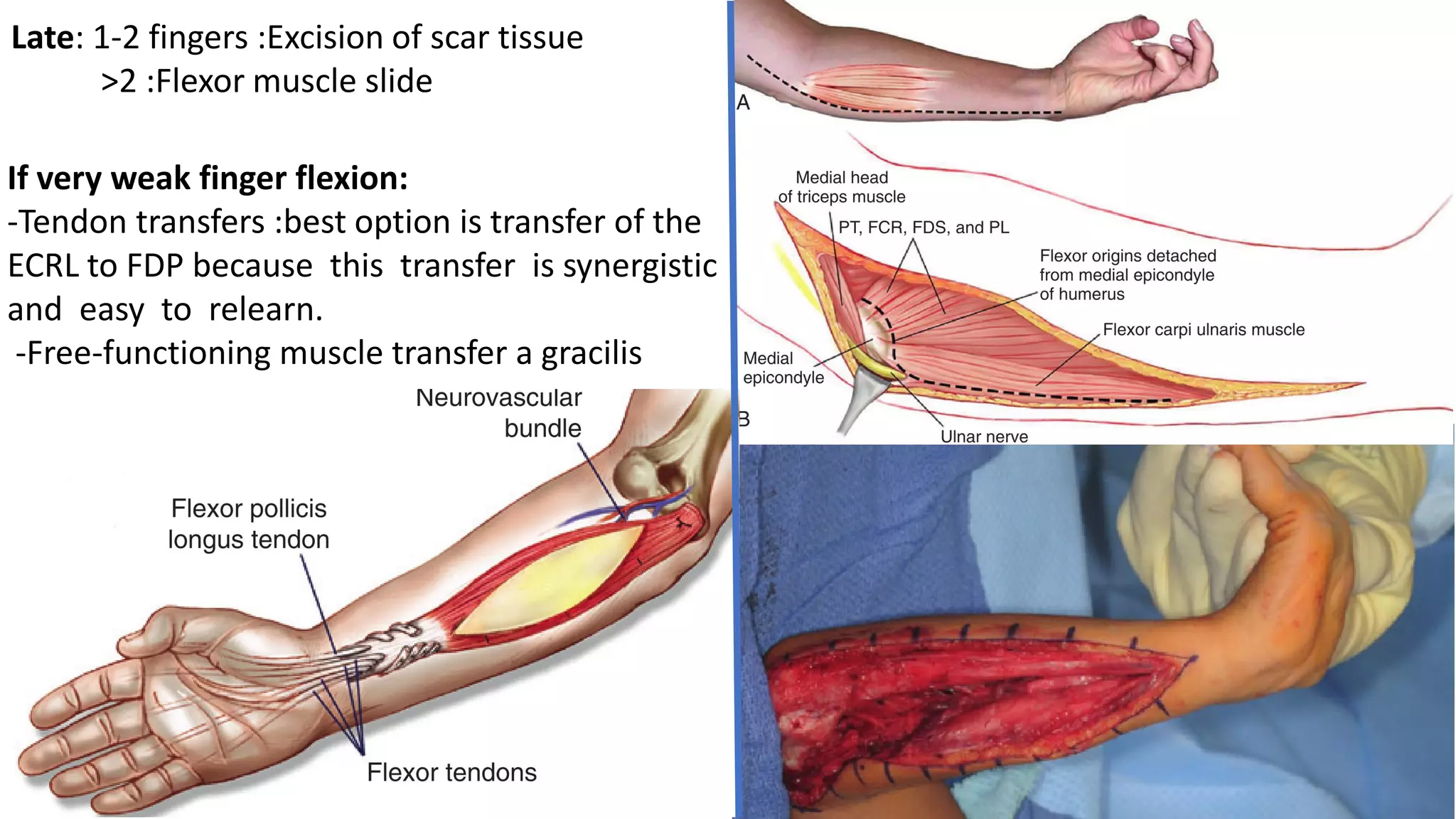
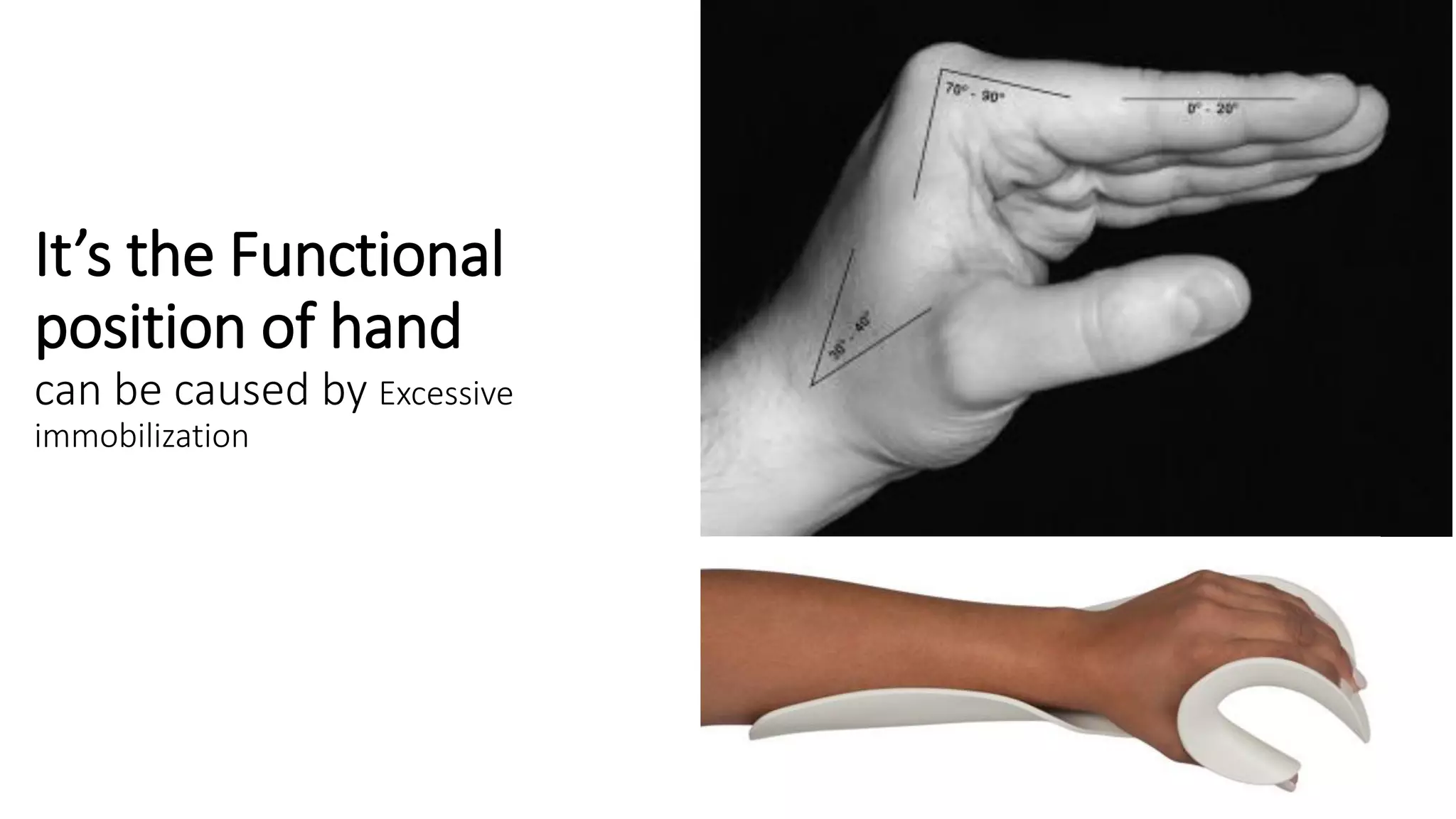
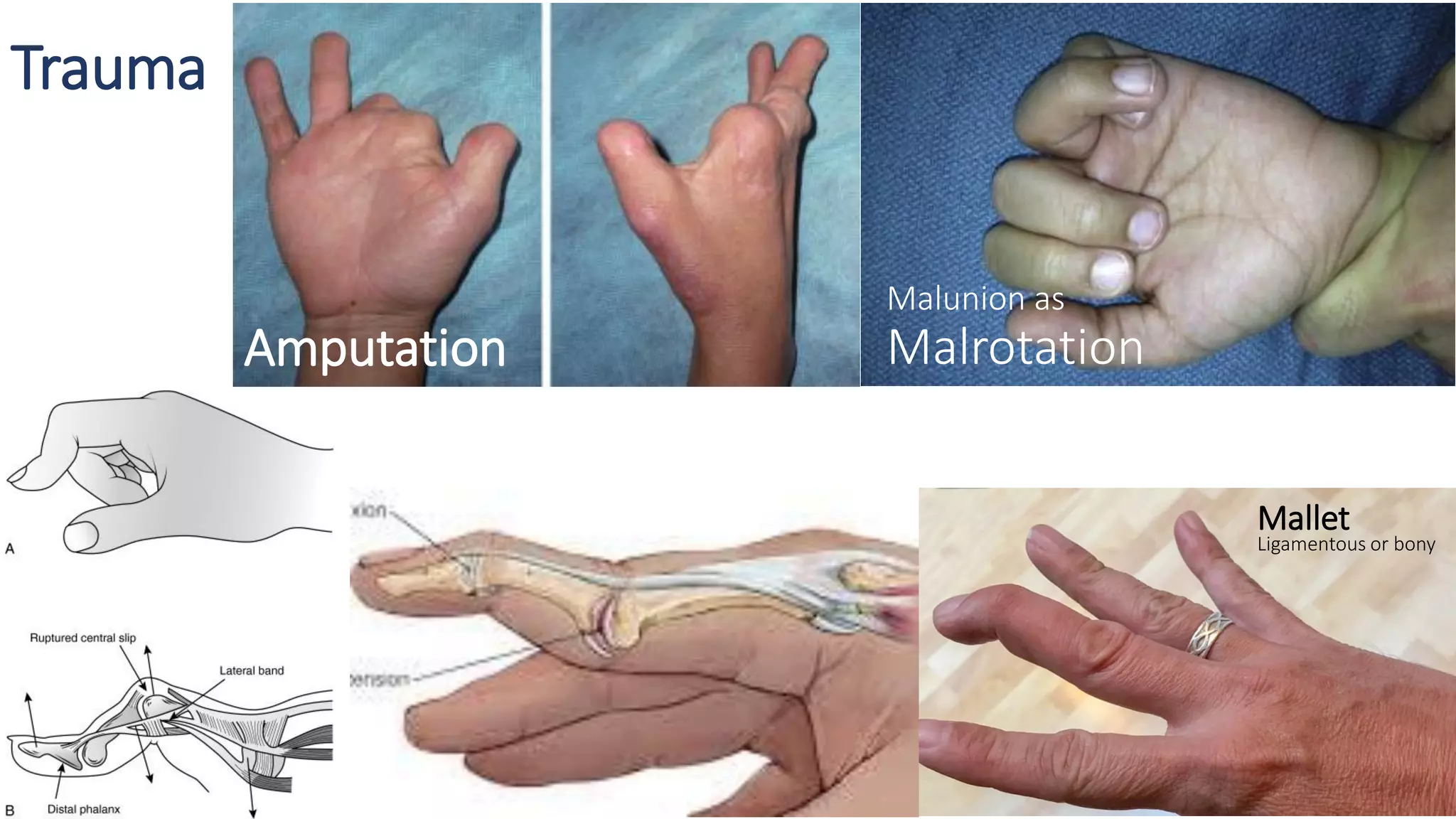
The document discusses various types of hand deformities including congenital deformities and those acquired through nerve injury, vascular injury, trauma, tumors, and inflammation. Key acquired deformities mentioned include Volkmann contracture resulting from prolonged ischemia, rheumatoid arthritis deformities like ulnar drift and Boutonniere deformity, and Dupuytren's contracture caused by thickening of the palmar fascia. Management approaches are described for different conditions, including tendon transfers, splinting, synovectomy, and fasciectomy.