Download to read offline



1) Habits can be classified in various ways such as oral habits, oral hygiene habits, adverse habits, and dietary habits. Common oral habits include thumb sucking, tongue thrusting, mouth breathing, bruxism, lip biting, nail biting, and cheek biting. 2) Maintaining good oral hygiene through proper brushing, flossing, using mouthwashes and rinses, and a balanced diet can help prevent dental caries, gingivitis, and periodontitis. Adverse habits like smoking and tobacco chewing increase the risk of oral cancer and periodontal disease. 3) A balanced diet with a variety of nutrients is important for overall health. Dietary habits like the









































































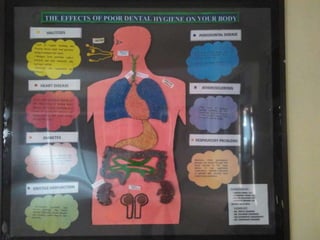
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
