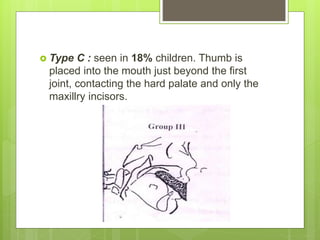
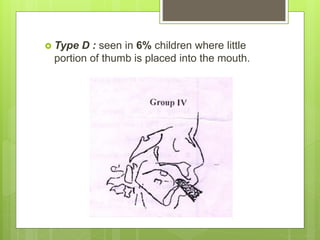
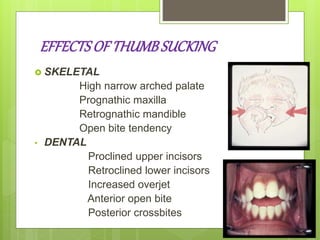
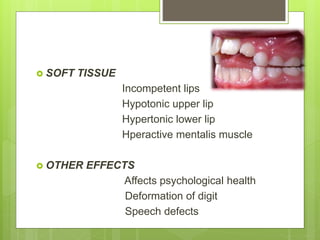
The document discusses various oral habits that can affect dental development, including thumb sucking, tongue thrusting, mouth breathing, bruxism, and lip biting. It defines each habit, discusses classifications, potential etiologies, effects on dental occlusion and facial growth, diagnosis, and treatment approaches. Common treatment involves identifying and addressing the underlying cause, interrupting the habit through various appliances, and correcting any resulting malocclusion. Psychological counseling may also be used for habits stemming from emotional factors. A multidisciplinary approach is often needed to successfully manage pernicious oral habits.


![Bruxism
RAMFFORD[1966]
BRUXISM IS THE HABITUAL
GRINDING OF TEETH WHEN THE
INDIVIDUAL IS NOT CHEWING OR
SWALLOWING](https://image.slidesharecdn.com/98ebab9a-e7e0-4816-86ce-6eb84e512a50-160607165439/85/HABITS-36-320.jpg)