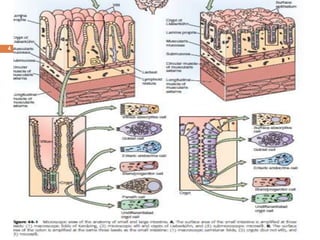
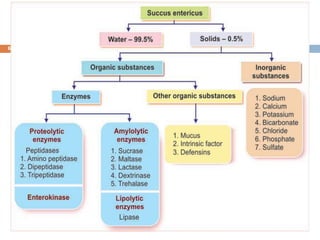
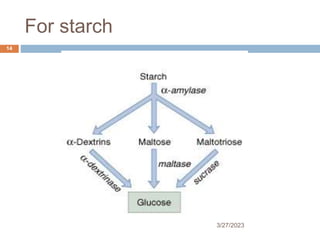
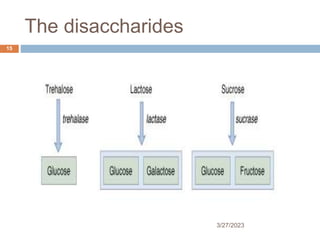
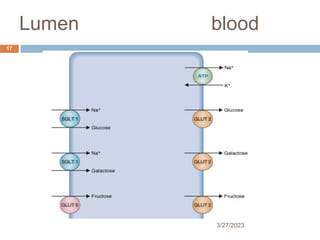
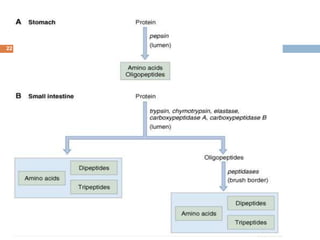
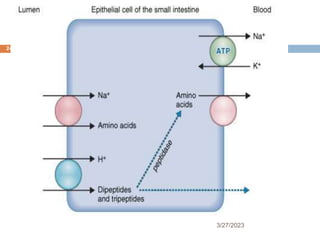
The document provides an overview of digestion and absorption processes in the small and large intestines, detailing the roles of various enzymes and secretions. It highlights the journey of carbohydrates, proteins, and lipids from ingestion to absorption, including disorders like lactose intolerance and pancreatic insufficiency. Additionally, it discusses the absorption of vitamins and minerals, fluid balance, and mechanisms leading to diarrhea.