GERD.pdf
•
0 likes•30 views

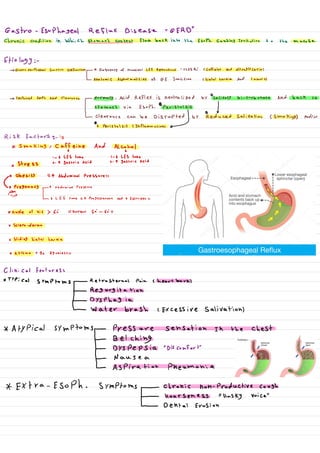
Gastroesophageal reflux disease (GERD) is caused by gastric acid irritating the esophagus. It is often due to transient lower esophageal sphincter relaxations that allow acid to flow back into the esophagus. Risk factors include smoking, caffeine, alcohol, obesity, pregnancy, hiatal hernia, and medications. Symptoms include heartburn, regurgitation, dysphagia, and atypical symptoms like chest pressure or cough. Diagnosis involves testing like endoscopy and pH monitoring if symptoms persist after trial of proton pump inhibitor treatment or if high risk complications are present. Treatment focuses on lifestyle changes and acid suppression with proton pump inhibitors or H2 blockers.

Recommended
More Related Content
Similar to GERD.pdf
Similar to GERD.pdf (20)
More from عباس مشتاق
More from عباس مشتاق (19)
Recently uploaded
Recently uploaded (20)
GERD.pdf
- 1. Gastroesophageal flux DiseaseRessoph. causing irritation to the masae Etiology:- -> Gastroesophageal Junction Dysfunction - ↑ Frequency of transient LES Relaxations " TLESR,"(Caffeine And Nitroglycerin) LanatomiC Abnormalities of of Junction Chiatal hernia And tumors) - > Impaired Esoph. Acid Clearance - Normally, Acid Reflex is neutralized by salivary bi-carbonate and back to Lstomach via Esoph. O peristalsis ↓ pearance,canbedisrupted by reduced Salination (smokings andare S Risk factors- is * smoking, caffeine And Alcohol A 1 - 6 LES tone 1- 6 LES tone x stress -- A gastric Acid 2- ↑ gastric Acid x obesity ↑ Abdominal Pressures * Pregnancy ↑ Abdominal Pressure -I - Lo LES fone 4 Progesterone And 4 Estrogen *Angle of his 6: normal 50-60 X Sclero-derma x sliding hiatal hernia * Asthma B2 Agonists Clinical features: * Typical symptoms - Retrosternal Pain (heartburn) ↓ Regurgitation - _ ° Dysphagia L water brash, excessive salivations * Atypical symptoms - Pressure sensation in the chest ↓ Belching - DYSPCPSia "Discomfort" L Nause a - ↳ Aspiration Pheumonia * Extra-Esoph. symptoms - chronic non-productive cough I Hoarseness Husky voice" - Dental Erosion
- 2. Aggravating factors: - ~ Ling Down shortly After meals * certain foods/beverages Red flags 8 Anemia And/or GS Bleeding" hematemesis, hematochezia " 0 weight loss o vomiting * Male ·Presence of 71 Risk for Barrett esoph. *rees, soy ~ obe se * SYMP1oms>5Y * European Decent Diagnosis:- - There is no gold standard test for the Dx of GERD. - If Patient with chest pain -> ECG + Cardiac Enzyme "troPonin" -> Normal - Patient with suspecte GERD Without Red flags or high Risk of Barrett Esoph. Start with once-Daily PPI for 8 * If relief symptoms of GERD - can stop PPI * If Persist symptoms or Recur After stop PPI or Red flags or High Risk for Barrett ESOPL. -> E6D A esoau. Monitoring * If Erosive will see by ↳ measure so. PH over 24-48 h using telemetry capsule catheter - PH -> Abnormal "Nor-crosise Reflux Disease" I X treat by PPI for 8 W - With Normal EGD And PH treat by Low Dose PPI or H2 Antagonists -I
- 3. ↑ reatment :- * Initial with lifestyle changes And Acid suppression therapy ppy, Hz Antagonist. * Surgical therapy" is not Routinely indicated"(fundoplication() 18: Dor fundo. !27 Toupet fundo. 360 complete fund. "Nissen fundoplication" complication.. B arrett Esophages "Intestinal metaplasia of the ESOPL. mucosa IDA - mucosal erosion and ulceration - Chronic Bleeding- Anemia Esophageal stricture = SoPhageal Ring "Schatzki Rings" Aspiration pneumonia Reflux laryngitis Hoarsenesss) * St -