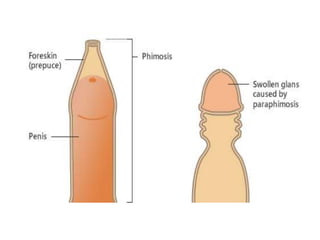
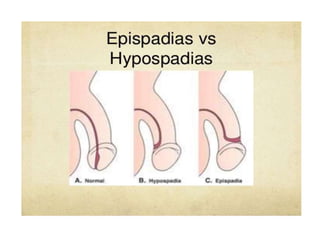
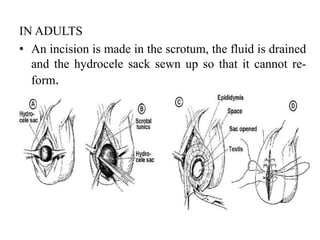
This document discusses various genitourinary disorders including urinary incontinence, phimosis and paraphimosis, epispadias and hypospadias, and hydrocele. It defines each condition, describes causes, presentations, assessments, and treatments. Urinary incontinence has several types defined by the circumstances that cause urine leakage. Phimosis and paraphimosis involve the foreskin becoming too tight or retracted. Epispadias and hypospadias are birth defects where the urethra opening is abnormal. Hydrocele is a fluid collection in the scrotum around the testes. Surgical and medical treatments aim to correct abnormalities and symptoms for each condition.