This document discusses gastrointestinal intubation, including:
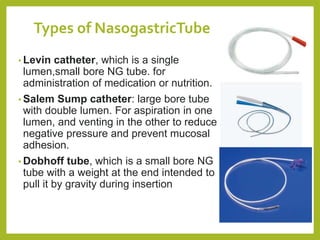
- Types of gastrointestinal intubation like orogastric, nasogastric, and nasointestinal tubes.
- Common uses of gastrointestinal intubation like administering medications, sampling sections for diagnostics, and performing lavage.
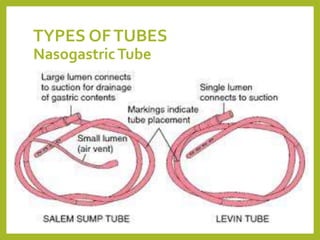
- Types of tubes used like orogastric, nasogastric, and nasointestinal tubes, some with multiple lumens.
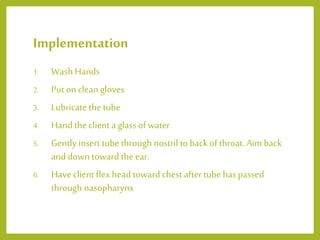
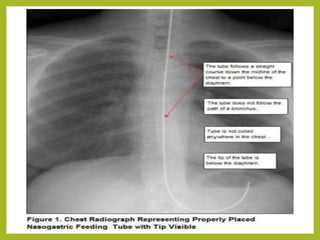
- The technique for nasogastric intubation including positioning, measuring tube length, lubricating the tube, and having the patient swallow to advance the tube into the stomach.