DEFFINITION
• Acute diarrheais defined as sudden onset of excessively loose stools
of >10ml/kg/day in infants and >200g/24 hours in older children
which lasts less than 14 days
• When episode lasts longer than 14 days – chronic diarrhea/ persistent
diarrhea
3.
• Increase inthe frequency of the stool
• Increase in the fluidity of the stool
• Increase in the weight of the stool
• Normal stool output : 5gm/kg/day
• Diarrhea: 10gm/kg/day
4.
WHAT IS NOTDIARRHOEA ?
• Frequent passage of small stools
• Passage of pasty stools in a breast fed infant
• Passage of watery stools in newborn infant after 3-4 days of birth
• Passage of stools immediately or during feeding
5.
CLASSIFICATION
• DEPENDING ONDURATION
• Acute diarrhea- upto 2 weeks
• Chronic diarrhea- >2 weeks
• Persistent diarrhea- >2 weeks – infective
• Protracted diarrhea > 2 weeks with malnutrition
• DEPENDING ON SITE OF PATHOLOGY
• Small bowel diarrhea
• Large bowel diarrhea
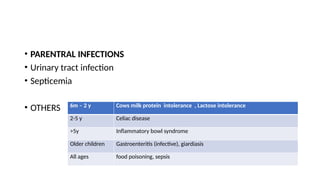
• PARENTRAL INFECTIONS
•Urinary tract infection
• Septicemia
• OTHERS 6m – 2 y Cows milk protein intolerance , Lactose intolerance
2-5 y Celiac disease
>5y Inflammatory bowl syndrome
Older children Gastroenteritis (infective), giardiasis
All ages food poisoning, sepsis
10.
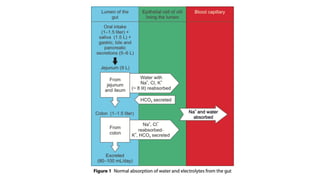
PHYSIOLOGICAL DISTURBANCE INDIARRHEA
• Total body water : ECF and ICF
• ECF
• 20-25% of body weight
• 5% plasma and 15% interstitial fluid
• Sodium and chloride – anions
• ICF
• 30-40% of body weight
• Potassium – cation
12.
• Diarrheal lossmainly from ECF
• Replacement with fluids rich in sodium with lower potassium
• TYPES OF DEHYDRATION
• Isonatremic – most common : 70-80%
• Hyponatremic – rare : 10-15%
• Hypernatremic – very rare - <5%
17.
COMPENSATORY MECHANISM
• lossof water and electrolytes in diarrheal stools, leads to increase in
• renin
• angiotensin
• aldosterone
• antidiuretic hormone (ADH)
• fall of glomerular filtration rate (GFR)
• retention of water by these mechanisms results in isotonic or hypotonic
dehydration
• Pre-existing or uncorrected potassium deficiency
19.
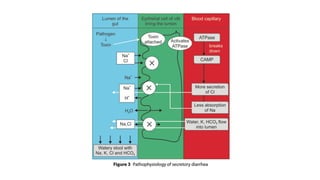
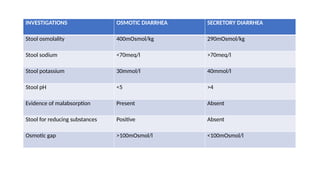
• SECRETORY DIARRHEA
•Acute watery diarrhea with profound losses
• Losses of water and electrolytes
• Sodium pump failure
• Rapid development of dehydration and electrolytes imbalance
• Common – ETEC, cholera
20.
• OSMOTIC DIARRHEA
•Injury to enterocytes may result brush border damage and epithelial
destruction
• Leading to reduced disaccharidase activity
• Large, explosive and acidic stools
21.
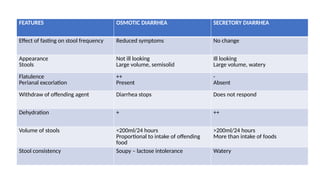
FEATURES OSMOTIC DIARRHEASECRETORY DIARRHEA
Effect of fasting on stool frequency Reduced symptoms No change
Appearance
Stools
Not ill looking
Large volume, semisolid
Ill looking
Large volume, watery
Flatulence
Perianal excoriation
++
Present
-
Absent
Withdraw of offending agent Diarrhea stops Does not respond
Dehydration + ++
Volume of stools <200ml/24 hours
Proportional to intake of offending
food
>200ml/24 hours
More than intake of foods
Stool consistency Soupy – lactose intolerance Watery
DYSENTRY
• Intestinal mucosalcells are invaded by micro-organisms
• Inflammatory reaction
• Presenting with blood and mucus
• More prone to develop : intestinal perforation, toxic megacolon,
rectal prolapse
24.
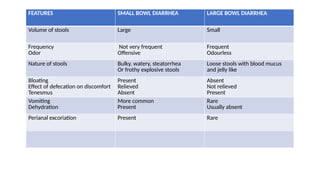
FEATURES SMALL BOWLDIARRHEA LARGE BOWL DIARRHEA
Volume of stools Large Small
Frequency
Odor
Not very frequent
Offensive
Frequent
Odourless
Nature of stools Bulky, watery, steatorrhea
Or frothy explosive stools
Loose stools with blood mucus
and jelly like
Bloating
Effect of defecation on discomfort
Tenesmus
Present
Relieved
Absent
Absent
Not relieved
Present
Vomiting
Dehydration
More common
Present
Rare
Usually absent
Perianal excoriation Present Rare
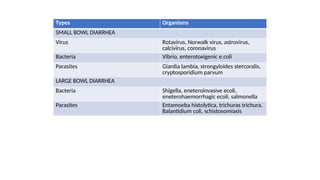
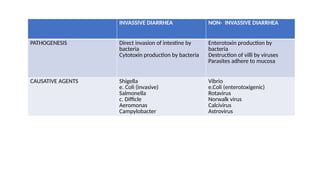
INVASSIVE DIARRHEA NON-INVASSIVE DIARRHEA
PATHOGENESIS Direct invasion of intestine by
bacteria
Cytotoxin production by bacteria
Enterotoxin production by
bacteria
Destruction of villi by viruses
Parasites adhere to mucosa
CAUSATIVE AGENTS Shigella
e. Coli (invasive)
Salmonella
c. Difficle
Aeromonas
Campylobacter
Vibrio
e.Coli (enterotoxigenic)
Rotavirus
Norwalk virus
Calcivirus
Astrovirus
27.
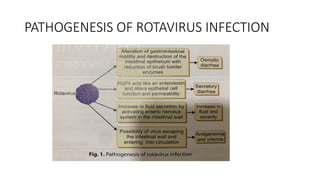
PATHOGENESIS OF ROTAVIRUSDIARRHEA
• OSMOTIC DIARRHEA
• Enterocyte damage leads to lactose malabsorption
• SECRETORY DIARRHEA
• Crypt cell proliferation – increased secretion of electrolytes and water
• NSP4 production – increased intracellular calcium, chloride secretion
• Neuromediate vascular ischaemia – neurotransmitter release
28.
• OSMOTIC ANDSECRETORY DIARRHEA
• Inflammation – rotavirus infected enterocytes activate nuclear factor
and produce chemokines
• HYPERMOTILITY DIARRHEA
• Stimulation of auerbach plexus
• INCREASED GUT PERMIABILITY
• Antigen antibody complex
PATHOGENESIS OF CHOLERA
•Organism adheres to small bowel epithelium – epithelium remains
intact
• ENTEROTOXIN – binds to ganglioside receptor
• Increased production of CAMP
• Massive purging of electrolyte rich sodium, chloride, bicarbonate and
potassium
31.
HISTORY TAKING
• AGE– infants <3m should be treated at hospital
• GENDER - toddlers diarrhea is chronic, non-specific, boys
• RESIDENCE – cholera : epidemics, food poisoning
• CHIEF COMPLAINTS – fever for 3 days, loose stools for 3 days
• HOPI
Onset, duration, frequency
Stools – consistency, volume (small/large)
Character – frothy/ oily/ sticky to pan
Associated with blood or mucus
H/o bottle feeding
Worms in stools
Drug exposure
32.
• Precipitating andrelieving factors
• Co-existing symptoms
Vomiting –
number of episodes, times of onset after food intake
Content of vomitus
Abdominal pain
Fever
Tenesmus
Lethargy, refusal of feeds, abnormal movements
33.
• Abdominal distension
•Features of dehydration – excessive thirst, drowsiness
• Bladder history - urine output, burning during urination
• Oral intake – amount and type of feeds during illness
• h/o drug intake
34.
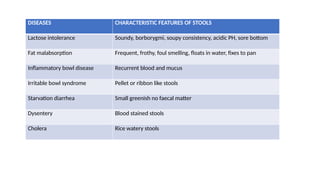
DISEASES CHARACTERISTIC FEATURESOF STOOLS
Lactose intolerance Soundy, borborygmi, soupy consistency, acidic PH, sore bottom
Fat malabsorption Frequent, frothy, foul smelling, floats in water, fixes to pan
Inflammatory bowl disease Recurrent blood and mucus
Irritable bowl syndrome Pellet or ribbon like stools
Starvation diarrhea Small greenish no faecal matter
Dysentery Blood stained stools
Cholera Rice watery stools
• TREATMENT HISTORY
•h/o hospitalization
• h/o drugs – antibiotics, antineoplastic
• h/o radiation
• h/o native treatment
• CONTACT HISTORY – tuberculosis
• ANTENATAL – newborn
• BIRTH HISTORY –
• pre term prone to infections and breast milk intolerance
• Mode of delivery - vaginal – more prone – aspiration of organisms
37.
• NEONATAL –LBW, pre maturity, birth asphyxia
• Umbilical cord catheterization – sepsis
• GROWTH
• Growth retardation – chronic diarrhoea, malabsorption , protracted diarrhea
• IMMUNISATION history : rotavirus and typhoid
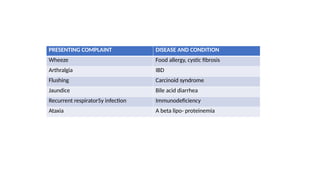
• FAMILY AND SIBLING HISTORY –
• Acute - food poisoning – time interval and onset
• Chronic- malabsorption syndrome, celeiac disease, inflammatory bowl diseases, celiac
disease, food allergy
• jaundice –chronic liver disease
• Chronic cough – cystic fibrosis
38.
• NUTRITIONAL HISTORY
•Diet during before and during onset of illness
• Food allergy or intolerance to food
• Wheat - celiac disease
• Sugar – sucrose isomaltase deficiency
• Affect of w/h food
• Cows milk
• SOCIOECONOMIC HISTORY
• Water and sanitation facility
39.
• GENERAL EXAMINATION
•Consciousness: normal, altered, unconscious
• General appearance: child looks ill
• Nutritional status- under nourished/ well nourished
• Signs of nutritional deficiency :
• Acrodermatits enteropathica – zinc deficiency
• Dermatitis – pellagra
• Vitamin D deficiency – malabsorption syndrome : bossing, aloplecia
• Vitamin A deficiency - malabsorption syndrome
40.
• SIGNS OFDEHYDRATION –
• Depressed AF
• Sunken eyes
• Absence of tears
• Dry tongue
• ASSOCIATED FEATURES
• pallor
• Jaundice
• Clubbing – celiac disease, IBD
• Lymphadenopathy - leukemia, lymphoma
• Erythema nodosum – IBD
• Pedal edema – PEM, protein loosing enteropathy
• Perianal excoriation
• Oral cavity – oral thrush – immunodeficiency
• Skin – purpura ecchymosis – DIC (septecemia, thrombocytopenia, HUS)
• Scratch marks – bile acids – steatorrhea
• Hands – white nails – protein loosing eneteropathy
41.
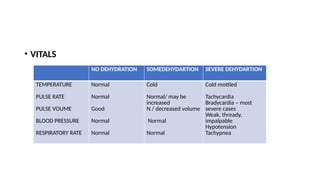
• VITALS
NO DEHYDRATIONSOMEDEHYDARTION SEVERE DEHYDARTION
TEMPERATURE
PULSE RATE
PULSE VOUME
BLOOD PRESSURE
RESPIRATORY RATE
Normal
Normal
Good
Normal
Normal
Cold
Normal/ may be
increased
N / decreased volume
Normal
Normal
Cold mottled
Tachycardia
Bradycardia – most
severe cases
Weak, thready,
impalpable
Hypotension
Tachypnea
42.
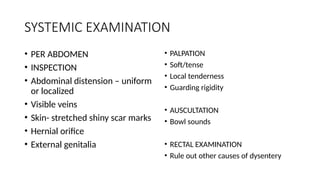
SYSTEMIC EXAMINATION
• PERABDOMEN
• INSPECTION
• Abdominal distension – uniform
or localized
• Visible veins
• Skin- stretched shiny scar marks
• Hernial orifice
• External genitalia
• PALPATION
• Soft/tense
• Local tenderness
• Guarding rigidity
• AUSCULTATION
• Bowl sounds
• RECTAL EXAMINATION
• Rule out other causes of dysentery
43.
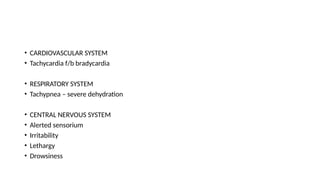
• CARDIOVASCULAR SYSTEM
•Tachycardia f/b bradycardia
• RESPIRATORY SYSTEM
• Tachypnea – severe dehydration
• CENTRAL NERVOUS SYSTEM
• Alerted sensorium
• Irritability
• Lethargy
• Drowsiness
44.
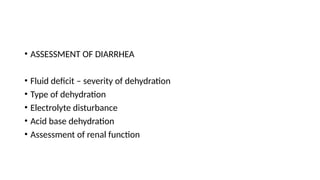
• ASSESSMENT OFDIARRHEA
• Fluid deficit – severity of dehydration
• Type of dehydration
• Electrolyte disturbance
• Acid base dehydration
• Assessment of renal function
45.
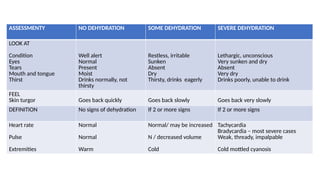
ASSESSMENTY NO DEHYDRATIONSOME DEHYDRATION SEVERE DEHYDRATION
LOOK AT
Condition
Eyes
Tears
Mouth and tongue
Thirst
Well alert
Normal
Present
Moist
Drinks normally, not
thirsty
Restless, irritable
Sunken
Absent
Dry
Thirsty, drinks eagerly
Lethargic, unconscious
Very sunken and dry
Absent
Very dry
Drinks poorly, unable to drink
FEEL
Skin turgor Goes back quickly Goes back slowly Goes back very slowly
DEFINITION No signs of dehydration If 2 or more signs If 2 or more signs
Heart rate
Pulse
Extremities
Normal
Normal
Warm
Normal/ may be increased
N / decreased volume
Cold
Tachycardia
Bradycardia – most severe cases
Weak, thready, impalpable
Cold mottled cyanosis
46.
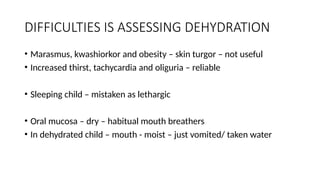
DIFFICULTIES IS ASSESSINGDEHYDRATION
• Marasmus, kwashiorkor and obesity – skin turgor – not useful
• Increased thirst, tachycardia and oliguria – reliable
• Sleeping child – mistaken as lethargic
• Oral mucosa – dry – habitual mouth breathers
• In dehydrated child – mouth - moist – just vomited/ taken water
47.
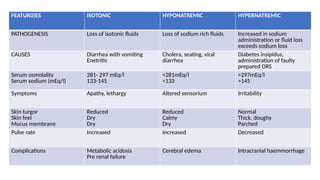
FEATUR0)ES ISOTONIC HYPONATREMICHYPERNATREMIC
PATHOGENESIS Loss of isotonic fluids Loss of sodium rich fluids Increased in sodium
administration or fluid loss
exceeds sodium loss
CAUSES Diarrhea with vomiting
Enetritis
Cholera, seating, viral
diarrhea
Diabetes insipidus,
administration of faulty
prepared ORS
Serum osmolality
Serum sodium (mEq/l)
281- 297 mEq/l
133-145
<281mEq/l
<133
>297mEq/l
>145
Symptoms Apathy, lethargy Altered sensorium Irritability
Skin turgor
Skin feel
Mucus membrane
Reduced
Dry
Dry
Reduced
Calmy
Dry
Normal
Thick, doughy
Parched
Pulse rate Increased Increased Decreased
Complications Metabolic acidosis
Pre renal failure
Cerebral edema Intracranial haemmorrhage
48.
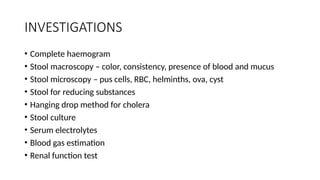
INVESTIGATIONS
• Complete haemogram
•Stool macroscopy – color, consistency, presence of blood and mucus
• Stool microscopy – pus cells, RBC, helminths, ova, cyst
• Stool for reducing substances
• Hanging drop method for cholera
• Stool culture
• Serum electrolytes
• Blood gas estimation
• Renal function test
DEFINITIONS
• Dehydration -Loss of water and dissolved salts from the body, occurring, for
instance, as a result of diarrhoea.
• Rehydration - The correction of dehydration.
• Oral Rehydration Therapy (ORT) - The administration of fluid by mouth to
prevent or correct the dehydration that is a consequence of diarrhoea.
• Oral Rehydration Salt (ORS) solution - Specifically, the complete, new
WHO/UNICEF formula.
51.
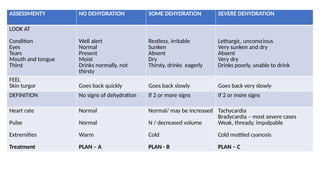
ASSESSMENTY NO DEHYDRATIONSOME DEHYDRATION SEVERE DEHYDRATION
LOOK AT
Condition
Eyes
Tears
Mouth and tongue
Thirst
Well alert
Normal
Present
Moist
Drinks normally, not
thirsty
Restless, irritable
Sunken
Absent
Dry
Thirsty, drinks eagerly
Lethargic, unconscious
Very sunken and dry
Absent
Very dry
Drinks poorly, unable to drink
FEEL
Skin turgor Goes back quickly Goes back slowly Goes back very slowly
DEFINITION No signs of dehydration If 2 or more signs If 2 or more signs
Heart rate
Pulse
Extremities
Treatment
Normal
Normal
Warm
PLAN – A
Normal/ may be increased
N / decreased volume
Cold
PLAN - B
Tachycardia
Bradycardia – most severe cases
Weak, thready, impalpable
Cold mottled cyanosis
PLAN – C
54.
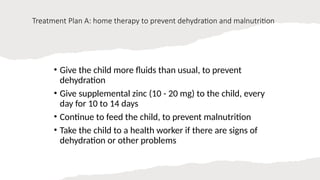
Treatment Plan A:home therapy to prevent dehydration and malnutrition
• Give the child more fluids than usual, to prevent
dehydration
• Give supplemental zinc (10 - 20 mg) to the child, every
day for 10 to 14 days
• Continue to feed the child, to prevent malnutrition
• Take the child to a health worker if there are signs of
dehydration or other problems
55.
SUITABLE FLUIDS
• Fluidsnormally containing salt
• ORS
• Salted drinks – salted rice water or salted yogourt drink
• Vegetable/ chicken soup with salt
56.
• HOME BASEDORS
• Salt sugar solution
• 3g – salt
• 18g – sugar
• 1 liter of water
57.
HOME AVAILABLE FLUIDS
NOTCONTAINING SALT UNSIUTABLE FLUIDS
Plain water
Rice water – unsalted
Soups – unsalted
Green Coconut water
Yoghurt drinks without salt
Unsweetened fresh fruit juice
Simple sugar solution
Glucose solution
Carbonated soft drinks
Fruit juice – tinned/ fresh
Gelatin deserts
Tea/ coffee
58.
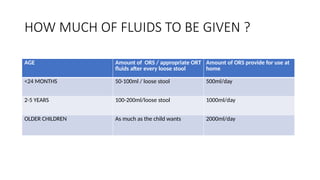
HOW MUCH OFFLUIDS TO BE GIVEN ?
AGE Amount of ORS / appropriate ORT
fluids after every loose stool
Amount of ORS provide for use at
home
<24 MONTHS 50-100ml / loose stool 500ml/day
2-5 YEARS 100-200ml/loose stool 1000ml/day
OLDER CHILDREN As much as the child wants 2000ml/day
59.
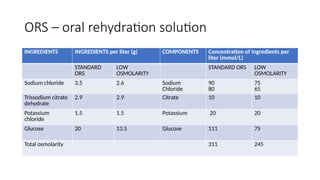
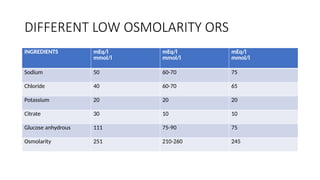
ORS – oralrehydration solution
INGREDIENTS INGREDIENTS per liter (g) COMPONENTS Concentration of ingredients per
liter (mmol/L)
STANDARD
ORS
LOW
OSMOLARITY
STANDARD ORS LOW
OSMOLARITY
Sodium chloride 3.5 2.6 Sodium
Chloride
90
80
75
65
Trissodium citrate
dehydrate
2.9 2.9 Citrate 10 10
Potassium
chloride
1.5 1.5 Potassium 20 20
Glucose 20 13.5 Glucose 111 75
Total osmolarity 311 245
60.
• balanced glucose-electrolytemixture, first used in 1969
• 1984, another mixture containing trisodium citrate instead of sodium
bicarbonate - improving the stability of ORS in hot and humid
climates.
• adverse effects of hypertonicity on net fluid absorption. This was
done by reducing the solution’s glucose and salt (NaCl)
concentrations.
61.
• glucose facilitatesthe absorption of sodium (and hence water) on a
1:1 molar basis in the small intestine;
• sodium and potassium are needed to replace the body losses of these
essential ions during diarrhoea (and vomiting)
• citrate corrects the acidosis that occurs as a result of diarrhoea and
dehydration.
62.
Properties of ORS-citrate
•stability in tropical countries where - up to temperatures of 60°C - no
discoloration occurs.
• A shelf-life of 2-3 years can be assumed without any particular storage
precautions.
• Reduces stool output especially in high output diarrhea
• Increases intestinal absorption of fluids and electrolytes
DISADVANTAGE OF STANDARDORS
• Poor acceptable due to taste
• Increased volume, purge rate and duration of diarrhoea
• High sodium concentration
Dangerous in edematous children
Congestive cardiac failure – anemia
• Risk of hypernatremia
66.
ADVANTAGE OF LOWOSMOLARITY ORS
• Treatment of ADD in newborn and young
• Effective water and sodium absorption
• Less stool output and reduced frequency of vomiting
• No risk of developing hypernatremia
• More stability of reconstituted solution
• Decreases number of hospitalizations
• Single formula would be promoted for all age
67.
SUPER ORS
• Cookingrice for 20 minutes and then adding salt
• During digestion glucose is absorbed slowly and promotes sodium
absorption
• Puffed rice can also be used
• 50-60gm of rice is used
• Glucose polymers or amino acids – glycine, alanine or glutamine can
be used
• Improves absorption of fluids and electrolytes
68.
• ADVANTAGE
• Tastesbetter
• More calories
• Culturally acceptable
• Reduces diarrhea by adding more substrate to gut lumen without
increasing osmolality
• SUPER SUPER ORS – adding zinc to super ORS
69.
• ORS FORTIFIEDWITH AMINO ACIDS
• L- alanine and glycine, glutamine : high osmolarity
• Efficacious in cholera
• ZINC FORTIFIED ORS
• Modifies the course of diarrhoeal illness
• Decreases the severity of diarrhea
• Prevents recurrent episodes of diarrhea
70.
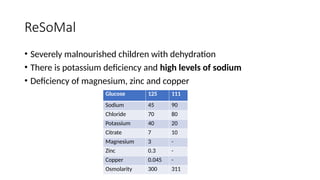
ReSoMal
• Severely malnourishedchildren with dehydration
• There is potassium deficiency and high levels of sodium
• Deficiency of magnesium, zinc and copper
Glucose 125 111
Sodium 45 90
Chloride 70 80
Potassium 40 20
Citrate 7 10
Magnesium 3 -
Zinc 0.3 -
Copper 0.045 -
Osmolarity 300 311
72.
• It issupplied as powder in satchets.
• Previously 1 satchet was reconstituted by adding 2 L of water to each
satchet therefore producing 2L of rehydration solution
• In order to not waste the quantity of prepared solution UNICEF in
2010 reduced satchet size to 50%
• New satchets are added to 1 L of water
• Can also be prepared by diluting one ORS in 2L of water and adding
25g/L of sucrose and 20ml/L of mineral mix
73.
• ReSoMal isgiven 5ml/kg every 30 minutes for 2 hours orally or with
NG tube
• 5-10ml/kg/hr for next 4-10 hours ,excat amount to be given is
determined by –how much the child wants
-stool loss
-vomiting
Replace ReSoMal doses at 4,6,8, and 10 hours with F-75 if rehydration
is continuing
Continue feeding with F-75
74.
PRECAUTIONS WHILE GIVINGORS
• High fiber diet should be avoided along with ORS
• Should be given in small sips – preferably with spoon
• If there is vomiting – ORS should be given after 10 minutes
• If vomiting is severe – IV fluids should be given
• Staple food should be given
• Rice with milk, curd and sugar can be given
PLAN – A: treatment in NO DEHYDRATION
• Without any physical signs
• Fluid therapy
• Continued feeding
• Zinc supplementation
• Identification of danger signs
77.
WARNING SIGNS
• Highpurge rate
• Persistent severe vomiting/ frequent vomiting
• Marked thirst
• Refusal to eat/ drink
• Blood in stool
• Fever
• Child not getting better in 3 days
• Rice watery stools – cholera
• Anuria/ failure to pass urine >12 hours
• Altered sensorium/ drowsiness/ convulsions
78.
WHO Recommendations forZINC
• Children >6months 20mg elemental zinc daily
• Children 2-6months 10mg elemental zinc daily
• To be continued for 14 days
• Use zinc alone – sulfate/acetate/gluconate
• Avoid iron with zinc
• Once or twice daily
79.
ROLE OF ZINC
Causesof zinc deficiency
• Breast milk does not supply sufficient zinc after 6 months
• Inadequate food intake
• Poor intake of animal food
• High phytate content
• Increased fecal loss
80.
EFFECT OF ZINCDURING DIARRHEA
• Improves epithelial repair
• Increases activity of brush border enzymes
• Increases T cell immunity
• Regulation of water and electrolytes
• Reduces stool output
• Reduces the duration of diarrhea
• Prevents subsequent episodes next2-3 months
81.
Plan-B treatment ofSOME DEHYDRATION
• WHO ORS under supervision of medical staff over 4 hours
• In infants and severely malnourished – correction over 6 hours
• Replacement of ongoing losses : 10-20ml/kg for each loose stool
• Infants <6m – not breast fed – clear watery fluids + ORS to prevent
hypernatremia
• Reassessment at the end of 4 hours – managed accordingly
• Breast feds are continued
• Semi solid foods are started after completion of deficit replacement
82.
TREATMENT PLAN B
•Deficit replacement : 75ml/kg over 4 hours ORS
• Maintenance therapy
• ORS in volumes equal to diarrheal losses
• 10-20ml/kg – each loose stool continue till diarrhea stops
• Provision of normal daily fluid requirements
• Upto 10kg : 100ml/kg
• 10-20kg : 1000ml + 50ml/kg
• >20kg : 1500ml + 20ml/kg
83.
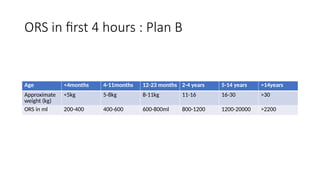
ORS in first4 hours : Plan B
Age <4months 4-11months 12-23 months 2-4 years 5-14 years >14years
Approximate
weight (kg)
<5kg 5-8kg 8-11kg 11-16 16-30 >30
ORS in ml 200-400 400-600 600-800ml 800-1200 1200-20000 >2200
84.
How to giveORS solution ?
• solution should be given to infants and young children using a clean
spoon or cup.
• Feeding bottles should not be used.
• For babies, a dropper or syringe (without the needle) can be used to
put small amounts of solution into the mouth.
• Children under 2 years of age should be offered a teaspoonful every
1-2 minutes
• older children may take frequent sips directly from the cup.
85.
• If thechild vomits, wait 5-10 minutes and then start giving ORS solution again, but more
slowly (e.g. a spoonful every 2-3 minutes).
• Reassesement of signs of dehydration
• If severe dehydration – IV fluids – severe dehydration
• If some dehydration – repeat plan B at the same time offer food and fluids as per plan A
• If no dehydration – considerfully hydrated when
• the skin pinch is normal;
- thirst has subsided;
- urine is passed;
- the child becomes quiet, is no longer irritable and often falls asleep.
•
86.
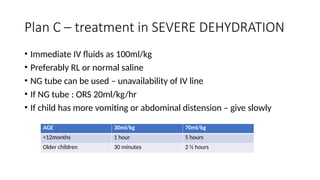
Plan C –treatment in SEVERE DEHYDRATION
• Immediate IV fluids as 100ml/kg
• Preferably RL or normal saline
• NG tube can be used – unavailability of IV line
• If NG tube : ORS 20ml/kg/hr
• If child has more vomiting or abdominal distension – give slowly
AGE 30ml/kg 70ml/kg
<12months 1 hour 5 hours
Older children 30 minutes 2 ½ hours
87.
• 100ml/kg isgiven over 3-6 hours
• Severely malnourished – SLOWLY OVER 6 HOURS
• 30ml/kg : over 1 hour
• 70ml/kg : over 5 hours
• Reassessment of hydration status every 1-2 hours
• If does not improve give IV fluids more rapidly
• Start ORS 5ml/kg/hr – once child can drink
3-4 hours : infants
1-2 hours : older children
88.
• Reassess after3 hours and 6 hours
• Classify dehydration and manage accordingly
• Continuously assessed for urine output, electrolytes, blood urea and
serum creatinine and glucose levels
• Maintenance fluids
89.
ROLE OF ANTIMICROBIALS
•h/o passing blood and mucus in stools
• Cholera
• Amebiasis
• Giardiasis
• Pseudomembranous colitis
• Parenteral diarrhea
90.
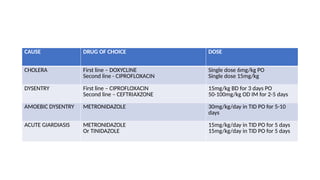
CAUSE DRUG OFCHOICE DOSE
CHOLERA First line – DOXYCLINE
Second line - CIPROFLOXACIN
Single dose 6mg/kg PO
Single dose 15mg/kg
DYSENTRY First line – CIPROFLOXACIN
Second line – CEFTRIAXZONE
15mg/kg BD for 3 days PO
50-100mg/kg OD IM for 2-5 days
AMOEBIC DYSENTRY METRONIDAZOLE 30mg/kg/day in TID PO for 5-10
days
ACUTE GIARDIASIS METRONIDAZOLE
Or TINIDAZOLE
15mg/kg/day in TID PO for 5 days
15mg/kg/day in TID PO for 5 days
91.
PROBIOTICS
• Living micro-organismthat confer health benefit on the host by
improving its intestinal microbial balance
• CHARACTERISTICS
• Live microbial feed supplements
• Compete with pathogens for micronutrients
• Naturally colonized in human gut
• Safe – no side effects
• Able to survive in GIT with beneficial effects
92.
BENEFICIAL EFFECTS
• Increaseresistance to infectious disease of intestine
• Decreases the duration of diarrhea
• Decreases flatulence
• Improve digestion
• Synthesis of vitamins : biotin and vitamin K
• Aid absorption of minerals : calcium and magnesium
93.
EFFECT ON PATHOGENICMICRO-ORGANISMS
• Modification of toxins
• Modification of toxin receptors
• Enhance immune response to pathogens
• Production of antimicrobial substance
94.
EFFECT ON HOSTMICRO-ORGANISMS
• Production of strong acids : lactic acid
• Metabolizing toxins
• Fragmenting and decreasing sludge – reducing concentration of
ammonia, sulphides
• Producing wide variety of antibiotic substance: acidophillin,
bacteriocin
PRE-BIOTICS
• These arenon-digestible food stuff that selectively stimukate growth
and activity of beneficial bacteria in gut
• Promote proliferation of bifido bacteria in colon
• Immune stimulation – reduces duration and incidence of bacteria
• Examples
• Fructo and galacto oligosaccharides
• Inulin
• Galactose
97.
SYNBIOTICS
• Combination ofprobiotics and prebiotics
• Health enhance g and health promoting – functional food
• ADVANTAGES
• Anticarcinogenic
• Antimicrobial
• Antidiarrheal
• Immunomodulation
• Decreases lipid activity
• Help decrease blood activity
• Suppress putrefactive process in stomach
98.
OTHER DRUGS INDIARRHEAL DISORDERS
• ANTIMOTILITY DRUGS : loperamide are contraindicated
Stagnation of fluids – harmful bacteria multiply – prolonging illness
• Adsorbents – kaolin and pectin : avoided
• Antisecretory agents : racecadotril : avoided
• Prebiotics and probiotics can be used
99.
RACECADOTRIL
• Enkephalinase inhibitor
•Reduces intestinal secretion by preventing breakdown of endogenous
enkephalins
• Reduces 48 hours stool output in acute watery diarrhea
100.
NUTRITIONAL MANAGEMENT INDIARRHEA
• foods suitable for a child with diarrhoea are the same as those required by
healthy children.
• MILK
• Infants of any age who are breastfed should be allowed to breastfeed as often
and as long as they want. Infants will often breastfeed more than usual this
should be encouraged.
• Infants who are not breastfed should be given their usual milk feed (or
formula) at least every three hours, if possible by cup.
• Infants below 6 months of age who take breastmilk and other foods should
receive increased breastfeeding. As the child recovers and the supply of
breastmilk increases, other foods should be decreased.
101.
• OTHERFOODS
• 6months and older infants – if already on soft diet – cereals,
vegetables and other foods
• If child is >6m such foods are not given, then it should ne started
during diarrhea or soon after it stops
• Should be culturally accepted, readily available, have high content of
energy and micronutrients
• Should be well cooked, smashed easy to digest
102.
• Milk shouldbe mixed with cereals if possible 5-10ml of vegetable oil
• Meat, fish, egg should be given if available
• Foods rich in potassium, such as bananas, green coconut water and fresh fruit juice
are beneficial.
• Should be given every 3 or 4 hours – 6times/day
• Frequent small feedings
• continue giving the same energy-rich foods and provide one more meal than usual
each day for at least two weeks.
• If the child is malnourished, extra meals should be given until the child has regained
normal weight-for-height.
HYPERNATREMIA
• Serum sodium>145mEq/L
• Water loss >> electrolyte loss
• Movement of water from brain cells to ECF
• Formation of IDIOGENIC OSMOLES
• Increases osmolality within neurons
• ECF volume may fall rapidly once hypernatremia gets corrected
• Cause the movement of water from ECF to neurons CEREBRAL EDEMA
MANAGEMENT
• Restore intravascularvolume
• Normal saline: 20ml/kg over 20 minutes
• Determine corrections based on initial sodium concentration
• 145-157 – 24 hours
• 158-170 – 48hours
• 171-183 – 72 hours
• 184-196 – 84 hours
108.
• Fluids -5% dextrose + half normal saline (20mEq/l K)
• RATE – 1.25 TO 1.5 times
• Adjust flow on basis of clinical status and serum sodium concentration
Sodium decreases too rapidly
• Decrease the rate of IV fluid
• Increase the concentration of sodium in IV fluid
Sodium decreases too slowly
• Decrease sodium concentration of IV fluid
• Increase rate of IV fluid
• Replace on going loss
109.
HYPONATREMIA
• Serum sodiumconcentration <135mEq/l
• Occurs due to excessive salt and water loss from GI tract
• Extracellular hypo-osmolality and tendency to move water inside the cell
• Clinical features
• Nausea
• Difficulty in concentration
• Confusion
• Lethargy
• Agitation
• Headache
• Seizures
• Brain stem herniation – cerebral edema
110.
• Diarrhea –sodium loss 50mEq/L
• Sodium deficit = 0.6 X body weight (135- observed sodium)
• 3% saline
• Sodium correction not more than >12mEq/L
111.
DIFFICULT DIARRHEA
• Diarrheain newborn:
• s/o systemic sepsis or UTI
• Increased rick of dehydration and assessment is difficult
• Necessary to estimate serum electrolytes and rule out sepsis
• Breast feeding to be continued along with ORS
• Antibiotics are recommended in low birth weight and associated
infections
112.
DIARRHEA IN HIVINFECTED CHILDREN
• Higher mortality
• Cryptosporidum is common pathogen
• Recurrent episodes of acute watery diarrhea as well as persistent
diarrhea
• Complicated – immunological status, infection with opportunistic
infection associated with malnutrition
• ORT and other standard treatment
113.
DIARRHEA CONTROL PROGRAM
•Started in 1978 to reduce mortality and morbidity
• National Oral Rehydration Therapy (ORT) 1985-86 : management of
diarrhea under 5years
• Supplies ORS packets to the states being organized by central
government
• Twice a year 150 packets to all subcentres in the country
• Now integrated with RCH
114.
REFERENCE
• Nelson –21st
edition
• Paediatric gastroenterology and hepatology – RIYAZ
• WHO article – treatment of diarrhea
• IAP textbook of Paediatrics – 6th
edition
• Auruchamy Lakshmanaswamy
115.
• Next class- 27th
may
• Topic : approach to chronic diarrhea by Dr. Deena Kumari




















































![HEMODYNAMIC_MANAGEMENT_STRATEGIES_IN_PEDIATRIC_SEPTIC_SHOCK[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hemodynamicmanagementstrategiesinpediatricsepticshock1-240713175925-f73ebe7c-thumbnail.jpg?width=640&height=640&fit=bounds)



















