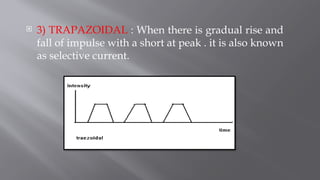
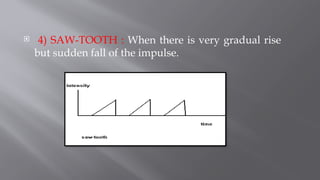
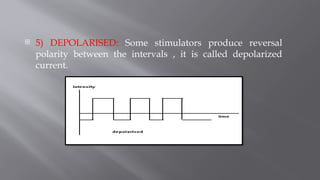
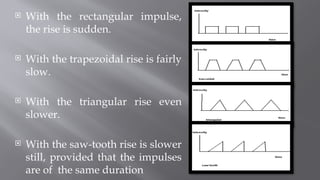
The document details the use and properties of galvanic current, a form of direct electric current used in therapeutic applications for muscle stimulation, especially in denervated muscles. It discusses different types of impulses (rectangular, triangular, trapezoidal, saw-tooth, and depolarized) and their effects on muscle contraction, the necessary adjustments in duration and frequency, and the methods of application in clinical settings. Additionally, it outlines the physiological effects, therapeutic benefits, contraindications, precautions, and instructions for proper treatment delivery.